
More Information
Submitted: 28 August 2020 | Approved: 04 December 2020 | Published: 07 December 2020
How to cite this article: Emiru TD, Birlie TA, Tasew SF, Amare AT, Tibebu NS, et al. How the COVID-19 outbreak affected physician-patient relationship. J Community Med Health Solut. 2020; 1: 026-034.
DOI: 10.29328/journal.jcmhs.1001004
Copyright License: © 2020 Emiru TD, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Client; COVID-19; DTGH; Ethiopia; KP
Abbreviation and acronyms: ARDS: Acute Respiratory Distress Syndrome; BBF: Blood and Body Fluid; COVID-19: Coronavirus Disease 2019; DTGH: Debre Tabor General Hospital; FMOF: Federal Ministry of Health; HCW: Health Care Worker; KAP: Knowledge, Attitude, and Practice; PPE: Personal Protective Equipment; SARS-Cov-2: Severe Acute Respiratory Syndrome Corona-2; WHO: World Health Organization

Assessment of knowledge, practice and associated factors towards prevention of novel corona virus among clients attending at Debre Tabor General Hospital, Debre Tabor Town, North West Ethiopia, 2020: Institutional based cross-sectional study
Tigabu Desie Emiru1*, Tekalign Amera Birlie2, Sheganew Fetene Tasew3, Abraham Tsedalu Amare2, Nigusie Selomon Tibebu1 and Chalie Marew Tiruneh1
1Department of Pediatric and Child Health Nursing, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
2Department of Compressive Nursing, College Of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
3Department of Emergency and Critical Care Nursing, College of Health Sciences, Debre Tabor University, Debre Tabor, Ethiopia
*Address for Correspondence: Tigabu Desie Emiru, Lecturer, Department of Pediatrics and Child Health Nursing, Debre Tabor University, P.O.Box: 272, Debre Tabor, Ethiopia, Email: [email protected]
Background: Corona virus disease is a highly infectious disease caused by the newly innovated corona virus. An emerging respiratory disease was abbreviated as COVID-19, after it has been first reported in December 2019 in Wuhan city of China. Ethiopia Ministry of health initiated multidisciplinary approach to tackle COVID-19 of which awareness creation is the main. The aim of this study is to assess knowledge, practice and associated factors towards prevention of novel corona virus among clients in Debre Tabor general hospital, Northwest Ethiopia, 2020.
Methods: Institution based cross sectional study design was conducted in Debre Tabor General hospital from May 15 to May 30, 2020. A structured questionnaire was used for data collection. The data were entered into epi data version 4.4 and exported to SPSS window version 25 for analysis. Binary and multivariable logistic regression was fitted. Odds Ratios with 95% Confidence interval and p - value ≤ 0.05 were considered to assert significance.
Result: A total of 345 clients were analyzed and the response rate was 96.4%. The mean age was 32.95 with S.D ± 13.18 years. Majority of the respondents were male (75.7%). Among the study participants 54.2% with (95% CI: [49.0, 59.2%]) and 49.0% with (95% CI: [43.5, 53.4%]) have good knowledge and god practice on COVID-19 preventions respectively. Sex AOR: 4.33 (2.06, 9.09), family size AOR: 2.49 (1.01, 6.15 and heard from social media AOR: 2.78 (1.21, 6.39) were significantly associated with knowledge of respondents. Knowledge AOR: 3.11 (1.59, 6.10) was significantly associated with practice of clients. Residency and those heard from TV were significant variables for both.
Conclusion and recommendation: In this study the overall knowledge and preventive practices of the respondents were found to be low. Sex, family size, residency and sources of information were associated factors for knowledge. In addition to this knowledge was significant factor for practice. Health education programs aimed at mobilizing and improving COVID-19 related knowledge and practice intend to be strengthened.
The virus itself in SARS-CoV-2, but the disease caused by that virus is called COVID-19. Corona virus disease is a highly infectious disease caused by the newly innovated corona virus [1]. The first cluster of this novel respiratory virus was reported from Wuhan province, China on 31, December 2019 even though retrospective studies identified appearance symptom in early December 2019. Evidences suggest that the virus is acquired from animals. However, the animal sourced or delivered the virus to humans is not absolutely identified [2].
Research studies done to identify the modes of transmission found that human to human transmissions mainly occur through respiratory droplets and direct contact with living or nonliving surface colonized by the novel corona virus [3,4].
Symptoms of COVID-19 may appear on infected patients after 2-14 periods of incubation. The most common symptoms of the disease are fever, cough, shortness of breath, and myalgia or fatigue. Patients may also have sore throat, and less commonly new loss of taste or smell, diarrhea and the like. Children are found to have mild infections than adults. Individuals having chronic illnesses like chronic respiratory disorders, heart problems, diabetes have higher chance of developing severe infections and complications from COVID-19 [5].
Currently various measures are being implemented to prevent transmission and spread of COVID-19 to individuals and communities. The most common recommended measures include frequent hand washing for at least 20 seconds, staying home, keeping physical distance, using personal protective equipment [6-8].
Different countries announced the problem to be a public health emergency at different times and on March 11, the world health organization declared that COVID-19 is a global pandemic [3].
Over 61,309,218 cases and 1,437,845 deaths were reported globally as of 27 November 2020 [9].
In Africa, over 2,134,290 cases and 51,033 deaths were reported until 27 November 2020. To time of data collection time 261 cases and 5 deaths reported in Ethiopia but now it accounts 107,669 total cases and 1,672 deaths in the country until 27 November 2020 [9]. There are confirmed cases of the virus in Ethiopia that found to have the problem while being treated for other medical problem. Individuals who neither have contact nor travel history were found to have the problem. This warns the spread of the virus to the community [10,11].
Intra hospital transmission of COVID-19 may occur in different ways. It may be from patient to patient, patient to health care professional and vice versa, health care professional to health care professional; patient attendants to patient attendant, patients, health care workers and vice versa. Patients, health care workers and patient attendants may also acquire the virus from contaminated inanimate materials like medical equipment, linen, chairs, and the like [12,13].
Patients coming to hospitals from urban and rural communities may bring corona to hospitals or transport the virus to their community from hospitals. Number of patients and attendants their physical distance and awareness about corona greatly affects the spread of the virus in hospitals [14-16].
Pandemic infections to and from hospitals can be prevented by collaborative efforts of health care workers, patients, patient attendants, hospital managers and other supportive staffs. Creating awareness about corona for patients and patient attendants coming from different communities is crucial and they can be used as vital instruments to deliver information related to COVID-19 when they return back to their village.
Even though the government is trying implementing preventive measures at different areas effectiveness and gaps are not well studied. Therefor this study investigated level of knowledge and practice of clients towards COVID-19 prevention, and factors affecting the preventive measure implementation process.
Study area and period
The study was conducted in Debre Tabor general hospital which is located in Debre Tabor. Debre Tabor is the capital city of South Gondar zone Amhara Regional state of Ethiopia. The climatic condition of the town is temperate and its average annual rain fall and temperature is 1553.7 mm and 150 degree Celsius respectively. DTGH was established by Dr. Yoganbik in 1923 E.C and totally under control by the government in 1969 E.C. it covers a total area of 94,725 m2 and more than 30 services delivered in the hospital. There are a total of 313 health professionals and 104 supportive staffs employed by the hospital. Besides, there are instructors and medical interns from Debre Tabor University College of medicine and health science, cleaners, security, and laundry workers from outsource serving the hospital. The study was conducted from May 15 to May 30, 2020.
Study design and participants characteristics
Institution based cross sectional study design was conducted in DTGH. All patients and their attendants in DTGH were considered as source population and the study population was selected patients and attendants in DTGH who fulfilled the inclusion criteria. Health care workers and hospital and unit manager who avail during the data collection period were included. All clients who avail during data collection period within the DTGH were included. However, clients who were mentally incompetent or critically ill or unable to give information during data collection were excluded from the study.
Sample size determination and sampling procedure
The sample size was determined by using single and double population proportion formula. To determine the knowledge and practice of clients’ single population proportion formula was used and the following assumptions were made during calculation. Knowledge of clients on COVID-19 was taken as 50% taking as P, 95% confidence level of certainty, and margin of error 5%. The sample size becomes:-
Where n = sample size needed
P = Knowledge of clients’ on COVID-19 Prevention
Z = Significance level at a confidence interval of 95% d = margin of error (0.05).
Z α/2 = value of the standard normal distribution corresponding to a significant level of alpha (α) 0.05 which is 1.96.
Since the source population is less than 10,000 correction formula was used to calculate the final sample size.
384/1 + 384/2150 = 325
Where n – final sample size and N- Source population (at that patient flow to the hospital in the previous month) [17]. By adding 10% (33) as non-response rate the final sample size was N=358.
Participants were selected randomly from each unit of the Hospital proportionally. Data were collected from different clients in found in different units of the hospital.
Variables of the study
Dependent variables
✓ Clients knowledge on COVID-19 prevention
✓ Clients practice on COVID-19 prevention
Independent variables
o Socio-demographic characteristics like:- Age, Sex, marital status, occupational status, educational status, family size, residences
✓ Hospital and individual related factors o Availability of personal protective equipment o Knowledge of clients on COVID-19 o Sources of information (TV, Radio, Social medias).
perational definitions
Knowledge on COVID-19 prevention: Eleven knowledge questions with forty seven responses were asked and correct answers were given score 1 and incorrect answers score 0; and a maximum score of 47 and minimum 0. Those having scored ≥ mean by categorizing the mothers as having good knowledge those who score less than the mean were classified as having poor knowledge.
Practice on COVID-19 prevention: Ten practice related questions with sixteen responses were asked and correct answers were given score 1 and incorrect answers score 0; and a maximum score of 16 and minimum 0. Those having scored ≥ mean by categorizing the clients as having good practice those who score less than the mean were classified as having poor practice.
Client: Is any hospital visitors age greater than 15 years whether the patient themself or their attendants in the hospital.
Data collection tool and techniques
Data was collected using structured interviewer administered questioner. All efforts were done to maintain two-meter distance between data collector and study participants and other preventive measures. The tool was translated to Amharic (local language) for easy understanding and translated back to English for analysis. Data quality was assured by trained data collectors, continuous supervision and daily checkup for content completeness and accurateness of the collected data.
Data processing and analysis
The data collected was entered to epi data version 4.4 and exported to SPSS version 25 software for analysis. Finally, the result was presented by graph, table and charts for the descriptive type of data. The association between each independent variable and the outcome variables was assessed by using binary logistic regression. All variables with p ≤ 0.25 in the binary logistic regression analysis were further taken to multiple logistic regression analysis in order to control all possible confounders. Adjusted odds ratio along with 95% CI and p - value < 0.05 were considered to declare factors that have statistically significant association with clients’ knowledge and practice towards COVID-19 prevention.
Ethical consideration
The ethical clearance was obtained from Debre Tabor University, college of medicine and health science research review committee. Then, supportive letter was submitted to hospital administrators. An oral and written informed consent was also provided to the study participants that they have the right not to be interviewed including the right to interrupt during an interview.
Socio-demographic characteristics of clients
Data of 345 clients were analyzed and the response rate was 96.4%. Among the participant, 132 (38.3%), were in age groups between 25 and 34 years with a median age of 30, mean of 32.95 and S.D ± 13.18 years. Majority of the respondents were male 261 (75.70%). About 46.1% of the respondents were single. Regarding family size of the respondents 30.1% was > 5. One hundred seven (15.9%) of the respondents were unable to read and write. Regarding occupational status, about one third (32.5%) were farmers (Table 1).
| Table 1: Socio-demographic characteristics of clients in DTGH, Ethiopia, 2020 (n = 345). | |||
| Characteristics | Category | Number | Percent |
| Sex | Male | 261 | 75.7 |
| Female | 84 | 24.3 | |
| Age (min = 17, max = 72, mean = 32.95, median = 30, SD = + 13.18) |
15-24 | 105 | 30.4 |
| 25-34 | 132 | 38.3 | |
| 35-44 | 44 | 12.8 | |
| 45-54 | 28 | 8.1 | |
| >55 | 36 | 10.4 | |
| Marital Status | Single | 159 | 46.1 |
| Married | 153 | 44.4 | |
| Divorced | 11 | 3.2 | |
| Widowed | 22 | 6.4 | |
| Family size | One | 47 | 13.6 |
| Two | 97 | 28.1 | |
| Three | 60 | 17.4 | |
| Four | 37 | 10.7 | |
| Five and above | 104 | 30.1 | |
| Residence | Urban | 176 | 51.0 |
| Rural | 169 | 49.0 | |
| Educational status | Unable to read and write | 55 | 15.9 |
| Read and write only | 58 | 16.8 | |
| Primary education | 77 | 22.3 | |
| Secondary education | 79 | 22.9 | |
| Diploma | 27 | 7.8 | |
| Degree and above | 49 | 14.2 | |
| Occupational status | Farmer | 112 | 32.5 |
| Merchant | 31 | 9 | |
| Government employee | 26 | 7.5 | |
| Housewife | 11 | 3.2 | |
| Student | 87 | 25.2 | |
| Daily labor | 78 | 22.6 | |
Client’s knowledge towards COVID-19 prevention
All most all of the respondents were heard about COVID-19 and 60 percent of them heard from health professionals (Figure 1). Most of the respondents 289 (83.8%) knew that COVID-19 is dangerous disease. Cough and Fever were the main symptoms answer by respondents 68.1% and 65.8% respectively (Table 2).
The overall knowledge of study participant this study revealed that only 187 (54.2%) of participants had good knowledge about COVID-19 prevention.
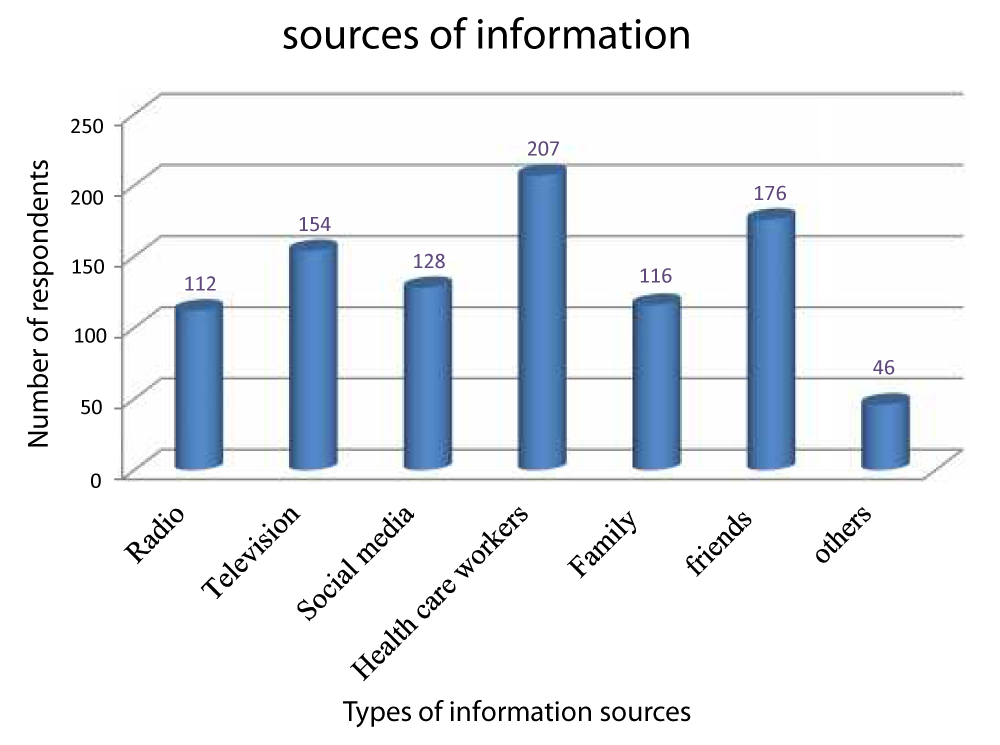
Figure 1: Types of information source about COVID-19 prevention of the respondents in Debre Tabor General Hospital, Debre Tabor, North West Ethiopia, 2020.
| Table 2: Respondents knowledge on COVID-19 prevention in DTGH, Debre Tabor, north west Ethiopia, 2020 (n = 345) | |||||
| s.no. | Variables | Responses | Number | Percent | |
| 1. | Have you ever heard about the new corona virus disease? | Yes | 335 | 97.1 | |
| No | 10 | 2.9 | |||
| 2. | What kind of information have you received about the disease? | How to protect yourself from the disease? | 322 | 93.3 | |
| Symptoms of the new coronavirus disease |
174 | 50.4 | |||
| How it is transmitted | 231 | 67.0 | |||
| What to do if you have the symptoms | 113 | 32.8 | |||
| Risks and complications | 31 | 9.0 | |||
| Other | 11 | 3.2 | |||
| 3. | How dangerous do you think the new coronavirus is? | Dangerous | 289 | 83.8 | |
| Not dangerous | 56 | 16.2 | |||
| 4. | Do you think you are at risk of getting sick with the new coronavirus? | Yes | 228 | 66.1 | |
| No | 117 | 33.9 | |||
| 5. | Who do you think is at highest risk to get the coronavirus? | Children under 5 years old | 101 | 29.3 | |
| Adolescents up to 15 years old | 61 | 17.7 | |||
| Anyone with serious underlying disease | 114 | 33.0 | |||
| Adults | 69 | 20.0 | |||
| Elderly persons | 124 | 35.9 | |||
| Pregnant women | 93 | 27.0 | |||
| Health workers | 83 | 24.1 | |||
| 6. | Do you know how the coronavirus is spread? | Droplets from infected people | 208 | 60.3 | |
| Airborne | 228 | 66.1 | |||
| Direct contact with infected people. | 198 | 57.4 | |||
| Touching contaminated objects/surfaces | 116 | 33.6 | |||
| Contact with contaminated animals | 10 | 2.9 | |||
| Don’t know | 62 | 18.0 | |||
| 7. | What are the main symptoms of COVID 19? | Fever | 227 | 65.8 | |
| Cough | 235 | 68.1 | |||
| Shortness of breath and breathing difficulties | 137 | 39.7 | |||
| Muscle pain | 58 | 16.8 | |||
| Headache | 89 | 25.8 | |||
| No symptoms | 33 | 9.6 | |||
| Don’t know | 98 | 28.4 | |||
| 8. | Do you know how to prevent becoming sick from the new corona virus? | Keeping physical distances | 198 | 57.4 | |
| Washing hands regularly using hand rub or soap and water | 288 | 83.5 | |||
| Avoid direct contact with frequently touched surfaces | 76 | 22.0 | |||
| Cover your mouth and nose when coughing or sneezing | 123 | 35.7 | |||
| 9. | From whom or what may you acquire corona infection in the hospital? | Health care workers | 103 | 29.9 | |
| Patients | 232 | 67.2 | |||
| Attendants | 238 | 69.0 | |||
| Cleaners | 99 | 28.7 | |||
| Linen, blanket, bed, mattress etc | 134 | 38.8 | |||
| Floor | 99 | 28.7 | |||
| Medical equipment | 99 | 28.7 | |||
| 10. | Who might you think bring the infection to your community? | Merchants | 96 | 27.8 | |
| Drivers | 131 | 38.0 | |||
| Individuals institution | who visit health | 74 | 21.4 | ||
| Individuals history to confirmed c | who had travel areas of corona ases | 241 | 69.9 | ||
| Health care workers | 41 | 11.9 | |||
| 11. | What has to be done to prevent the spread of coronavirus in your community? | Community education about corona | 270 | 78.3 | |
| Provision of personal protective equipment | 152 | 44.1 | |||
| Provision of materials for hand hygiene | 129 | 37.4 | |||
| Applying state of emergency | 189 | 54.8 | |||
Clients practice towards COVID-19 prevention
This study showed that only 169 (49.0%) of participants had good practice towards COVID-19 and its prevention. Based on our study result, 67.2% of respondents were wash their hands regularly using hand rub or soap and water, 71.3% of the respondents cover their mouth and nose when coughing or sneezing, only 44.9% of them using mask in and out of hospital and only 36.8 % of respondents were practicing avoid un protected direct contact with surfaces in repeated contact with humans (Table 3).
| Table 3: Respondents practice towards prevention of corona virus in DTGH, Debre Tabor, Northwest Ethiopia, 2020 (n = 345). | ||||
| s.no | Variables | Responses | Number | Percent |
| 1. | Do you wash your hands regularly using hand rub or soap and water? | Yes | 232 | 67.2 |
| No | 113 | 32.8 | ||
| 2. | Do you cover your mouth and nose when coughing or sneezing? | Yes | 246 | 71.3 |
| No | 99 | 28.7 | ||
| 3. | Do you avoid close contact with anyone? | Yes | 185 | 53.6 |
| No | 160 | 46.4 | ||
| 4. | Do avoid un protected direct contact with surfaces in repeated contact with humans? | Yes | 127 | 36.8 |
| No | 218 | 63.2 | ||
| 5. | Do you touch blood and body fluids without gloves? | Yes | 148 | 42.9 |
| No | 197 | 57.1 | ||
| 6. | Do you use masks in the hospital? Out of hospital | Yes | 155 | 44.9 |
| No | 190 | 55.1 | ||
| 7. | Do you cover your mouth and nose using your clothes? | Yes | 196 | 56.8 |
| No | 149 | 43.2 | ||
| 8. | Do you avoid touching your nose, mouth or face with your hands? | Yes | 168 | 48.7 |
| No | 177 | 51.3 | ||
| 9. | What would you do if you or someone from your family gets sick with the new coronavirus? | I would go to the hospital / health unit. | 275 | 79.7 |
| I would stay in quarantine | 138 | 40 | ||
| I will look for a more experienced relative to advise me on what to do |
19 | 5.5 | ||
| I'm going to look for the traditional healer | 8 | 2.3 | ||
| 10. | What will you do to prevent corona when you return back to your home? | Regular hand washing | 229 | 66.4 |
| Keeping physical distance | 236 | 68.4 | ||
| Creating awareness for friends and family members |
158 | 45.8 | ||
| Ventilating rooms | 55 | 15.9 | ||
Reasons not to comply with preventive practices
Majority 238 (68.99%) of the respondents’ report that crowding as a major reason for not complying with preventive practices towards COVID-19. Lack of awareness and lack of hand hygiene supplies were listed as other reasons of non-compliance as reported by 65.22% and 63.8% of clients respectively.
Factors associated with knowledge of clients towards prevention of COVID-19
Binary and multiple logistic regressions were used to identify variables significantly associated with clients’ knowledge towards prevention of COVID-19. All variables with p - value of < 0.25 in the binary logistic regression were taken in to multiple logistic regression. Variables with p - value of less than 0.05 in the multiple logistic regressions were considered significant.
In multivariable logistic analysis Sex of the respondents with AOR: 4.33 (2.06, 9.09) , family size AOR: 2.49 (1.01, 6.15), respondents residency AOR: 5.11 (2.40, 10.90), heard from TV AOR: 5.33 (2.43, 11.68) and heard from social media AOR: 2.78 (1.21, 6.39) were remained significantly associated with knowledge of respondents; with 95% CI and p - value of ≤ 0.05 (Table 4).
| Table 4: Bivariable and multivariable logistic regression analysis for knowledge by factors among clients in Debre Tabor General Hospital, Debre Tabor town, North West Ethiopia, 2020 (n = 345). | ||||||
| Variables | Category | Respondents Knowledge | Odd ratio (95% CI) | |||
| Good | Poor | Crude odds ratio | Adjusted odds ratio | p - value | ||
| Sex of the respondents | Male | 168 (64.5%) | 93 (35.6%) | 6.180 (3.49-10.93) | 4.326 (2.060-9.085) | 0.001** |
| Female | 19 (22.6%) | 65 (77.4%) | 1 | 1 | ||
| Family size | < 3 | 139 (68.1%) | 65 (31.9%) | 4.143 (2.63-6.54) | 2.491 (1.010-6.152) | 0.001* |
| > 4 | 48 (34.0%) | 93 (66.0%) | 1 | 1 | ||
| Residents of the respondent | Urban | 140 (79.5%) | 36 (20.5%) | 10.095 (6.14-16.60) | 5.114 (2.400-10.897) | 0.001** |
| Rural | 47 (27.8%) | 122 (72.2%) | 1 | 1 | ||
| Heard from radio | Yes | 72 (64.3%) | 40 (35.7%) | 1.85 (1.16-2.94) | ||
| No | 115 (49.4%) | 118 (50.6%) | 1 | 1 | ||
| Heard from TV | Yes | 125 (81.2%) | 29 (18.8%) | 8.97 (5.41-14.86) | 5.332 (2.434-11.680) | 0.001** |
| Heard from social media | No | 62 (32.5%) | 129 (67.5%) | 1 | 1 | |
| Yes | 108 (84.4%) | 20 (15.6%) | 9.433 (5.43-16.37) | 2.784 (1.212-6.395) | 0.001** | |
| No | 79 (36.4%) | 138 (63.6%) | 1 | 1 | ||
| Heard from friends | Yes | 112(63.6%) | 64(36.4%) | 2.193 (1.42-3.38) | ||
| No | 75(44.4%) | 94(55.6%) | 1 | 1 | ||
| Note: **significantly associated at "p ≤ 0.001": *Significantly associated at "p ≤ 0.05". 1 = Reference group | ||||||
Factors associated with clients’ practice towards prevention of COVID-19
Multiple regression analysis for clients level of practice with independent variables showed that clients. In multivariable logistic analysis knowledge of respondents AOR: 3.11 (1.59, 6.10), respondents residency AOR: 2.36 (1.05, 5.30) and those heard from TV AOR: 16.50 (7.57, 35.99) were remained significantly associated with the outcome variable (practice of clients) with 95% CI and p - value of ≤ 0.05 (Table 5).
| Table 5: Bivariable and multivariable logistic regressionanalysis for level of practice by factors clients in Debre Tabor GeneralHospital, Debre Tabor town, North West Ethiopia, 2020. (n =345). | ||||||
| Variables | Category | Respondents Practice | Odd ratio (95% CI) | |||
| Good | Poor | Crude odds ratio | Adjusted odds ratio | p - value | ||
| Knowledgeof respondents | Good | 135(72.2%) | 52(27.8%) | 9.468(5.764-15.553 | 3.111(1.587-6.099) | 0.001** |
| Poor | 34(21.5%) | 124(78.5%) | 1 | 1 | ||
| Familysize | <3 | 136(66.7%) | 68(33.3%) | 6.545(4.024-10.647) | ||
| >4 | 33(23.4%) | 108(76.6%) | 1 | |||
| Residencyof the respondent | Urban | 130(73.9%) | 46(26.1%) | 9.420(5.765-15.393) | 2.361(1.052-5.299) | 0.001* |
| Rural | 39(23.1%) | 130(76.9%) | 1 | 1 | ||
| Heardfrom TV | Yes | 133(86.4%) | 21(13.6%) | 27.269(15.178-48.992) | 16.503(7.566-35.99) | 0.001** |
| No | 36(18.8%) | 155(81.2%) | 1 | 1 | ||
| Heardfrom social media | Yes | 99(77.3%) | 29(22.7%) | 7.169(4.338-11.847) | ||
| No | 70(32.3%) | 147(67.7%) | 1 | |||
| Heardfrom family | Yes | 74(63.8%) | 42(36.2%) | 2.485(1.567-3.941) | ||
| No | 95(41.5%) | 134(58.5%) | 1 | |||
| Note:**Significantly associated at "p ≤ 0.001"; *Significantlyassociated at "p ≤ 0.05"; 1 = Reference group | ||||||
Muliticollinearity between knowledge and practice
In our study revealed that there was no muliticollinearity between knowledge and practice towards COVID-19 preventions (tolerance and VIF are 1.00). This indicates that there was no impact of knowledge on practice.
Still, the spread of COVID-19 is a major public issue in the world. So far no treatment or vaccine is open to it. Therefore, prevention is the best solution to control the spread and the impact of COVID-19. This study tried to assess the level of clients’ knowledge, practices and associated factors among clients in Debre Tabor general hospital. This study was conducted to fill the gap in the literature and providing a reference on KP among clients. We found that only around half of the participant (54.2%) with (95% CI: [49-59.2]) had good knowledge about COVID-19 related issues. This finding is consistent with a report by other study that (55.9%) of the study participants had good knowledge about COVID-19[18].
The current finding is higher than study on Knowledge and preventive practices towards COVID-19 early in the outbreak among Jimma University medical center visitors, Southwest Ethiopia overall knowledge of the visitors was 41.3% [19]. The discrepancy might due to increasing access to information and community awareness from time to time and also the spread of the virus becomes more rapid and address all of the world’s country that shows how the virus infectious and dangerous.
However, this study was much lower than the study done in at Addis Zemen hospital (66.1%) [20] and another study on KAP of COVID-19 among College Students in Amhara Region, Ethiopia 69.6% [21]. The difference might be the first study was done only on chronic patients and they may give more attention and also may have better exposure than other general clients. For the second it might be difference in the study population.
The study finding also much lower than the study conducted in health care workers of different setting of Ethiopia 88.2% of respondents had good knowledge [22]. This high percentage of knowledge about COVID-19 among healthcare workers is due to prolonged exposure to information since its global topic of discussion in the media and public. Another reason could be the effort of government and media in providing information starting from the time of the outbreak as well as heath is the prior concerns of health worker.
All most all of the respondents were heard about COVID-19 and we found that the majority 60% and 51.1% of the respondents found information from health professionals and friends respectively. In this study the 93.3 % of the study participant were heard how to protect them from the disease, 83.8% assumes it is dangerous and 66.1% says they are at risk of getting sick with the new coronavirus.
In this study sex of client was a significant contributor for knowledge of respondents. The odds of good knowledge was 4.33 folds in males [95% CI = (2.06, 9.09)] than females. It might be because mostly females participate in childcare, food preparation and other tasks compared with males. Therefore, information related to acquire knowledge regarding to COVID-19 is more likely to be addressed better among males by different information Medias.
Family size was another factor found significant for knowledge. The odds of good knowledge was 2.49 times higher in those family size less than or equal to three than those who had greater than or equal to four AOR: 2.49 (95% CI: 1.01, 6.15).
The odd of knowledge was five folds in those come from urban areas than rural clients AOR: 5.11 (95% CI: 2.40, 10.90). This is consistent with the study reports from Addis Zemen Hospital rural residence (AOR=19.0, 95% CI (6.87–52.66)) poor knowledge [20]. This is due to a lack of access to information in rural areas, where there is no electricity and mobile networks that help them to update themselves about COVID-19. Health information, which can improve patient knowledge and practice are becoming more accessible online; however it is not reachable to rural residents. Furthermore, rural residents in Ethiopia lack of access and health-promoting actions to prevent COVID-19.
The current study showed that there is a significant association between sources of information (Social media and television) and clients’ knowledge about COVID-19. It is also similar to the studies in Ethiopia, Vietnam and China [22,23]. Those who use social media as a source of information had about three times more chance of having good knowledge about COVID-19 and those use TV as a source of information five times more chance of having knowledge than others AOR: 2.78 (1.21, 6.39) and AOR: 5.33 (2.43, 11.68) respectively. This might be due to the use of global crises of outbreak social media platforms as a facilitator and distributor of COVID-19 related information for the world’s population during this critical time. As well as governmental and other agents use TV as source dissemination mode more of their tome to protect their population from the disease that showing visual and audio massages. We understand from this that social media is a great way of providing the latest updated information about this COVID-19 pandemic for individuals and the community.
This study showed that only 169 (49.0%) with (95% CI: [43.5-53.4]) of participants had good practice towards COVID-19 and its prevention. This is consistent with a study done at Addis Zemen Hospital [20]. Based on our study result, 67.2% of respondents were wash their hands regularly using hand rub or soap and water, 71.3% of the respondents cover their mouth and nose when coughing or sneezing, only 44.9% of them using mask in and out of hospital and only 36.8% of respondents were practicing avoid un protected direct contact with surfaces in repeated contact with humans. The possible reasons for these low preventive practices in the shortage of infrastructure, overcrowding and inadequate supply provided for the clients at the hospital.
In this study knowledge of respondents was a significant contributor for knowledge of respondents. The odd of good practices was three folds in those who had good knowledge than clients with poor knowledge AOR: 3.11 (1.59, 6.10). This is consistent with the studies conducted in different parts of Ethiopia [18-20]. This is if someone had good understanding about COVID-19 the level of preventive practice increases; therefore; emphasis better to give for the awareness creation and mobilization of the community.
The other predictors of the good level of practice on COVID-19 prevention was residency of the respondents. The odd of good preventive practice was two times more in urban respondents than rural with AOR: 2.36 (1.05, 5.30). this is consistent with the study conducted in Amhara, Ethiopia [21,24].
Those heard from TV AOR: 16.50 (7.57, 35.99) were rmained significantly associated with the good preventive practice on COVID-19. Moreover, this suggests further implementation, health promotion and community mobilization from the government is required for the application of good practice towards COVID-19 and its preventions.
Limitation
Attitude of the respondents was not studied here; moreover, the cross-sectional nature of the study did not allow us to show the cause-effect relationship.
In this study the overall knowledge and overall preventive practices of the respondents were found to be low. Sex of the respondents, family size, respondents’ residency and sources of information (heard from TV and heard from social media) were significantly associated with knowledge of respondents; and knowledge of respondents, respondents’ residency and those heard from TV were significantly associated with good preventive practice.
Health education programs aimed at mobilizing and improving COVID-19 related knowledge and practice are still rigorously needed that is easily understandable by all of the peoples, especially for those females clients and those from rural areas. Leaflets prepared in local languages should be administered for those having less media addressable country sides and health professionals at the health institutes should provide detailed information about COVID-19 to their patients. Concerned body better to give emphasis on strategies that helps to change the understanding of the population to prevent themselves from the virus.
Ethical approval and consent to participate
The ethical clearance was obtained from Debre Tabor University, college of medicine and health science research review committee. Then, supportive letter was submitted to hospital administrators. An oral and written informed consent was also provided to the study participants that they have the right not to be interviewed including the right to interrupt during an interview.
Availability of data and materials
Data will be available upon request from the corresponding author.
Authors’ contribution
Tigabu Desie Emiru, the corresponding author (PI), worked on supervising the data collectors, analyzing and interpreting the result and preparing the manuscript. The co-authors namely, Tekalign Amera, Sheganew Fetene, Abriham Tsedalu, Nugussie Solomon and Chalie Marew played their role in designing the study and training. Moreover, the co-authors wrote the manuscript. All authors were involved in reading and approving the final manuscript.
The authors acknowledged data collectors, and supervisors. The author is also deeply acknowledging Debre Tabor University. Last but not least, the respondents deserve sincere thanks for their kind responses.
- Tan W, Zhao X, Ma X. A novel coronavirus genome identified in a cluster of pneumonia cases — Wuhan, China. 2020.
- Global T, Alert O. Coronavirus disease 2019 ( COVID-19 ) Situation report -94. 2020.
- WHO. Global Surveillance for human infection with coronavirus disease (COVID-19). Interim Guid [Internet]. 2020; 27–29. https://www.who.int/publications-detail/global-surveillance-for-human-infection-withnovel-coronavirus-(2019-ncov)
- WHO. Modes of transmission of virus causing COVID-19_ implications for IPC precaution recommendations.
- WHO Global Surveillance for human infection with coronavirus disease (COVID-19) Interim Guid [Internet] 2020; 27–29. https://wwwwhoint/publications-detail/global-surveillance-for-human-infection-with-novelcoronavirus-(2019-ncov)
- Guan W, Chen R, Zhong N. Strategies for the prevention and management of coronavirus disease 2019. Eur Respir 2020; 55: 2000597. PubMed: https://pubmed.ncbi.nlm.nih.gov/32217658/
- WHO 2019 Novel corona virus strategic prepardness and response plan. 2020.
- Chughtaia AA, Khan W. Use of personal protective equipment to protect against respiratory infections in Pakistan_ A systematic review. J Infect Public Heal. 2019; 12: 522–527. PubMed: https://pubmed.ncbi.nlm.nih.gov/30738757/
- Worldometersinfo Coronavirus Update (Live) Worldometer 2020.
- Johns Hopkins Coronavirus Resource Center COVID-19 Map .
- Mandavilli A. Infected but Feeling Fine_ The Unwitting Coronavirus Spreaders.
- Modes of transmission of virus causing COVID-19 : implications for IPC precaution recommendations 2020; 19–21.
- Why Coronavirus Could Hit Rural Areas Harder - Lerner Center for Public Health Promotion – Syracuse University.
- Worldometersinfo Coronavirus Update (Live) Worldometer. 2020.
- Amid weak health systems WHO warns COVID-19 spreading to rural Africa 2020
- Abera Beyamo TD, Facha WF Compliance with standard precaution practices and associated factors among health care workers in Dawuro Zone, South West Ethiopia, cross sectional study _ BMC Health Services Research _ Full Text BMC Health Serv Res. 2019; 19.
- Debre AF. Tabor General Hospital. Unpublished. 2020.
- Dagne H, Alemu KA, Dagnew B, Taddesse D, Alemayehu AM, et al. Prevention Practice and Associated Factors of Coronavirus disease 2019 (COVID-19) Outbreak among Educated Ethiopians: An online Based Cross-sectional Survey. Res S©quare. 2020.
- Kebede Y, Yitayih Y, Birhanu Z, Mekonen S, Ambelu A. Knowledge, perceptions and preventive practices towards COVID-19 early in the outbreak among Jimma University Medical Ccenter visitors. Southwest Ethiopia PLoS ONE. 2020; 15: e0233744. PubMed: https://pubmed.ncbi.nlm.nih.gov/32437432/
- Akalu Y, Ayelign B, Molla MD. Knowledge, Attitude and Practice Towards COVID-19 Among Chronic Disease Patients at Addis Zemen Hospital, Northwest Ethiopia. Infect Drug Resist. 2020; 13: 1949–1960. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7322118/
- Tadesse AW, Melese N, Eshetie S, Chanie M, Ali A. Knowledge, Attitude, and Practice and Associated Factors towards COVID-19 among College Students in Amhara Region, Ethiopia; A Cross-Sectional Study. 2020.
- Jemal B, Ferede ZA, Mola S, Hailu S, Abiy S, et al. Knowledge, attitude and practice of healthcare workers towards COVID-19 and its prevention in Ethiopia: a multicenter study. 2020.
- Zhong BL, Luo W, Li HM, Zhang QQ, Liu XG, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biologi Sci. 2020; 16: 1745-1752. PubMed: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7098034/
- Aynalem YA, Akalu TY, Gebresellassie B, Sharew NT, Shiferaw WS: Assessment of undergraduate student knowledge, practices, and attitude towards COVID-19 in Debre Berhan University, Ethiopia.