
More Information
Submitted: August 11, 2021 | Approved: August 19, 2021 | Published: August 20, 2021
How to cite this article: Al Zahrani AM, Ali HM, Ahmed SA, Abdelakher AM, Al Zahrani AA, et al. Factors influencing referral delay of cancer patients to an oncology unit in the Southern Region of Saudi Arabia. J Community Med Health Solut. 2021; 2: 025-030.
DOI: 10.29328/journal.jcmhs.1001012
Copyright License: © 2021 Al Zahrani AM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Cancer; Delay; Complementary and alternative medicine; Cancer education; Cancer knowledge; Saudi Arabia

Factors influencing referral delay of cancer patients to an oncology unit in the Southern Region of Saudi Arabia
Ali M Al Zahrani1*, Hatim M Ali2, Shaza A Ahmed2, Ahmed M Abdelakher2, Asma A Al Zahrani3 and Hatoon Bakhribah1
1Medical Oncology Department, King Fahad Medical City, Riyadh, Saudi Arabia
2Medical Oncology Department, Armed Forces Hospital Southern Region, Khamis Mushait, Saudi Arabia
3Pharmaceutical Care Department, King Abdulaziz Medical City, Riyadh, Saudi Arabia
*Address for Correspondence: Ali Al Zahrani, MD, Medical Department, King Fahad Medical City, Riyadh, Saudi Arabia, Email: [email protected]
Introduction: Cancer treatment and prognosis depend heavily on early detection. Survival in the early stages is excellent for almost all types of cancer. Unfortunately, in Saudi Arabia, a large number of cancer patients present with advanced disease, resulting in a poor prognosis. There are three levels of delay in the management of cancer patients. The first level is the time between the first cancer-related symptoms and the presentation to the health facility, the second level is from the presentation to the diagnosis, and the third level is between the diagnosis and the treatment. This study aims to determine if there is a delay, at what level and to study the factors causing such delays.
Materials and methods: Two hundred cancer patients who presented to the Armed Forces Hospital Southern Region, Oncology Department, were interviewed from January 1st to June 30th, 2018. The interviews were conducted by trained physicians familiar with the questionnaire’s contents. The questionnaire consisted of four sections: a demographic section and three more sections to identify factors causing the delay at the three levels from the patients’ perspectives. All data were analyzed using the SPSS version 20.0.
Results: The mean patient age was 63 years. A total of 112 patients were female and 88 were male. The most common cancer type was breast cancer (27.5%). Among the patients, 61% were illiterate and 25.5% had elementary school degrees, 86% expressed little or no general medical knowledge about cancer. More women than men paid attention to cancer symptoms (70% vs. 54%). 75% of the patients presented to the first health facility after 2 months from the first appearance of symptoms (level 1 delay). Only 2% of the patients presented within one week. 50% of the patients received a diagnosis after visiting two health facilities. All patients were diagnosed at hospitals. 40% of patients used alternative medicines, 70% of whom thought this was the cause of their delayed presentations. 67% had their diagnosis confirmed within one month (level 2 delay), and 66% started their definitive treatment within one month (level 3 delay). 75% of the patients blame themselves for the delay. Educational level (p = 0.03), knowledge about cancer (p < 0.01), and the use of complementary and alternative medicines (CAM) (p = 0.01) were significantly associated with delayed presentation of patients to the health facility.
Conclusion: There is a delay in the presentation of cancer patients (level 1) in the southern part of Saudi Arabia. Educational level, knowledge of cancer symptoms, and use of complementary and alternative medicines are the main causes. There were no delays in diagnosis and start of treatment (level 2,3).
Cancer is a serious disease. It ranks second as the leading cause of death in most developed countries [1], and late presentation is one of the major factors contributing to a poor prognosis. According to the last Saudi Cancer Registry, more than 70% of patients present with the disseminated disease when treatment is of low benefit [2].
The health system in Saudi Arabia is still under development. It is fragmented, and there is no good primary health care system covering the whole country to date [3]. Many people still believe in unconventional cancer treatment, resulting in a high rate of complementary and alternative medical practices [4]. This might be a possible cause of the delay before definitive treatment. The stigma of cancer in some Arab countries causes some patients to hide their early symptoms or even deny them completely [5]. Moreover, some health professionals lack basic knowledge of how to recognize and deal with early signs and symptoms of cancer [6].
In our country, there is no national screening program for cancer, which makes cancer diagnosis to be delayed. An early cancer diagnosis is a key focus in disease control and treatment because there is a strong association between the time from symptom onset to diagnosis and both stages at diagnosis and subsequent survival [7]. According to SEER data from the USA (Surveillance, Epidemiology, and End Result program), survival from cancer is strongly related to an early presentation and stage of cancer [8].
The symptoms of cancer differ dramatically according to the type; however, in general, there are two main categories. First, those who present with ‘red flag symptoms (i.e., changes in a mole, a lump, or unusual bleeding) and those who have other symptoms. Patients presenting with ‘red flag symptoms’ have been categorized as having ‘delayed’ diagnosis if they did not present within one week of symptom onset, whilst patients reporting any other symptom have been categorized as having ‘delayed’ diagnosis if it took them longer than four weeks to present [9].
Others, mainly from developing countries, defined delays differently, but the delay is generally defined as a prolonged interval between discoveries of initial symptoms to a presentation by more than 12 weeks, as periods longer than this have been associated with poorer survival [10].
There are several possible reasons for the causes of delay in third world countries; some are related to the patients and some to health professionals, and others are related to the health system itself [11].
Most of the research on this topic was carried out in developed countries, and one systematic review of 19 studies identified a strong association with old age and some evidence of not recognizing the initial symptoms of cancer, hiding cancer symptoms, non-white ethnicity, and low education [12]. There is also substantial geographical variation due to differing social, cultural, and economic situations, especially between developed and developing countries; therefore, the results of studies from developed countries cannot be generalized to developing countries [13].
The delay in diagnosis was divided into three component intervals: the period from symptom recognition to the first consultation with a health care professional (termed as patient delay, level 1), the period from the first presentation to a health care professional to the initiation of investigations for cancer (physician delay and system delay, level 2), and the period from initiation of investigations to commencement of treatment (treatment delay, level 3).
The southern part of Saudi Arabia is heavily populated, and few hospitals offer comprehensive cancer management. Many people still believe in complementary and alternative treatments, and the causes of cancer are mainly attributed to non-medical reasons. The Oncology department in Armed Forces Hospitals Southern Region is a referral oncology unit that accepts patients from all over the southern areas.
During daily practice, it was noticed that many patients usually come in the late stages of cancer, where treatment would be of limited benefit. Therefore, this study was conducted to determine the delay period and the possible causes of delay in both diagnoses and treatment. Thus, this study examines the causes of cancer patients’ referral delay from different possible perspectives, including, patient factors, health care provider factors, and health care system factors at the three levels of delay; before the presentation to the health facility, after the presentation to the health facility to the diagnosis and from the diagnosis until the start of the treatment.
200 oncology patients who presented to the Armed Forces Hospitals Southern Region, Oncology Department from 1st January to 30th June 2018 were interviewed by physicians after obtaining informed consent. The physicians were fully aware of the content of the questionnaires and their purpose. A meeting was conducted with all physicians involved in obtaining the information to explain all items of the questionnaire. All authors had contributed to the whole process.
The questionnaire consisted of four sections. The first collects demographic data and the subsequent three more sections explore factors related to delay. The first of these sections identify the possible causes of the delay from the time of the first symptoms until the presentation to the first health facility. (i.e., patient delay - Level 1) The second section identifies the possible causes of the delay from the time of the first health facility visit to the time of the diagnosis of cancer (i.e., physicians’ and health system delays - Level 2). The third section identifies any factors that could contribute to the delay in starting treatment (i.e., from the diagnosis to the start of definitive cancer treatment - Level 3).
All the data were introduced to SPSS version 20.0.
Approval was obtained by the local ethical committee.
A total of 200 patients with cancer were interviewed. The mean age of the participants was 63 years; 112 patients were female and 88 were male and 51% were older than 60 years. The most common cancer was breast cancer (27.5%), followed by colorectal cancer (15%), and thyroid cancer (14%). Lung cancer had the lowest incidence rate (1%). It was found that 61% were illiterate while 25.5% had elementary school degrees only, and 86 % expressed little or no general medical knowledge about cancer.
More women than men paid attention to cancer symptoms (70% vs. 54%). This study identified a significant delay at level 1 (from the first symptom to presentation to the health facility - Figure 1) of more than 2 months, while there was no major delay in levels 2 and 3 i.e., diagnosis at the health facility and starting the treatment (Figures 2,3). Seventy-five percent of patients presented to the first health facility 2 months after the date of the first symptoms identified related to their cancer (level 1). Only 2% of patients presented within one week of the first symptoms (Figure 1 and Table 1), while 55% delayed their health facility visits because they did not think their symptoms indicated serious illness. Thirty percent used complementary and alternative medicines (CAM) and visited a local healer, and 70% of them thought this was the cause of their delayed presentations (Table 2).
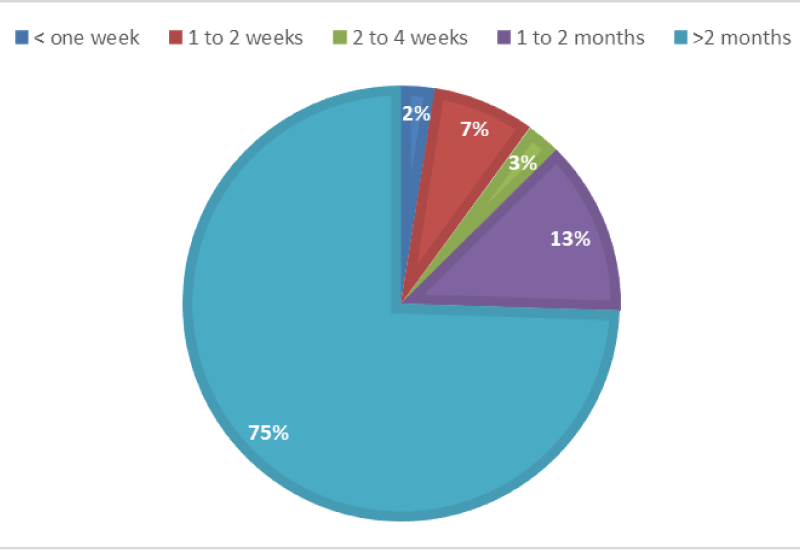
Figure 1: Level 1 delay (Time from 1st symptoms to reaching health facility).
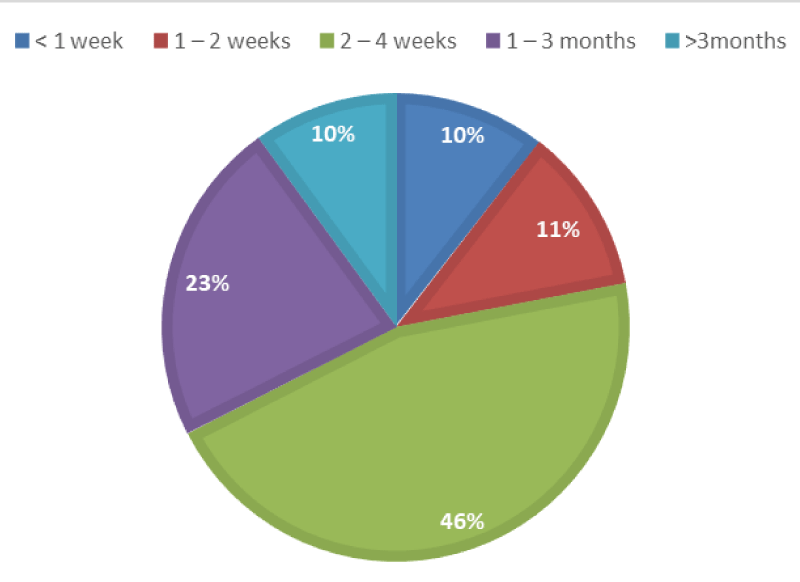
Figure 2: Level 2 delay (Time from reaching the health facility to diagnosis).
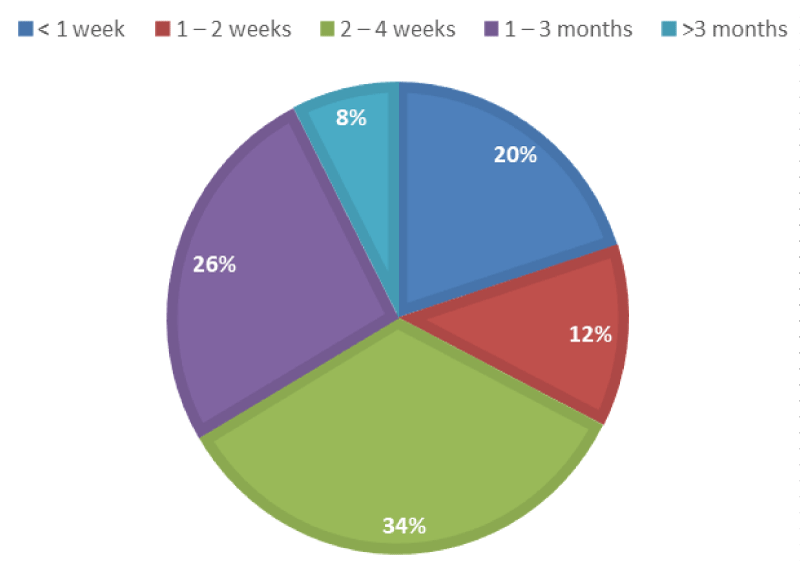
Figure 3: Level 3 delay (Time from Diagnosis to Treatment).
| Table 1: Relation between the time of referral and the presentation to the health facility. | ||||
| Time from thinking its cancer related to presenting to Health Facility | Total | Referral | Test | |
| Early | Late | p | ||
| N = 25 (%) | N = 175 (%) | |||
| < one week 1to 2 weeks 2to 4 weeks 1to 2 months > 2 months |
4 3 8 35 150 |
2(50) 3(100) 2(25) 9(25.7) 9(6) |
2(50) 0(0) 6(75) 26(74.3) 141(94) |
< 0.001** |
| **p ≤ 0.001 is statistically highly significant; χ2 Chi-squaretest for trend. | ||||
| Table 2: Relation between the time of referral and different causes. | ||||
| Delayin seeking health service | Total | Referral | Test | |
| Early | Late | p | ||
| N = 25 (%) | N = 175 (%) | |||
| Idon’t think it’s important Analternative advice Nohealth services around Prolongedappointments Alternativemedicine and local healers |
124 10 6 10 50 |
14(11.3) 2(20) 3(50) 4(40) 2(4) |
110(88.7) 8(80) 3(50) 6(60) 48(96) |
0.001** |
| χ2 Chi-square test; **p < 0.001 is statistically highlysignificant. | ||||
After visiting the health facility, 67% of patients had a confirmed diagnosis within one month, while only 10% had their diagnoses confirmed within one week (Figure 2). A total of 51.5% blamed themselves and relatives as the cause of their delayed diagnosis, while 36% blamed the health professionals. (Level 2 delay). Fifty percent of the patients were diagnosed after visiting two health facilities. Of all the cases diagnosed at hospitals, 95% of these diagnoses were made at tertiary hospitals. After diagnosis, 66% of patients started definitive treatment within one month (Figure 3). A total of 90.5% blame health professionals for their delay in starting treatment. (Level 3).
Educational level (p = 0.03) (Table 4), knowledge about cancer (p = 0.01) (Table 3), and the use of alternative medicines, visiting local healers, alternative advice, and system failure (p = 0.001) were also significantly associated with delay in presentation of patients to the health facility (Table 2).
| Table 3: Relation between the time of referraland level of patient knowledge about cancer. | ||||
| Knowledge | Total | Referral | Test | |
| Early | Late | p | ||
| N = 25 (%) | N = 175 (%) | |||
| Nothing Little Fair Good Excellent |
75 60 38 21 6 |
3(4) 11(19.3) 3(8) 2(10) 6(100) |
72(96) 49(81.7) 35(92) 19(90) 0(0) |
0.01* |
| χ2 Chi-square test for trend *p = 0.01 isstatistically significant. | ||||
| Table 4: Relation between the time of referraland level of patient education. | ||||
| Level of education | Total | Referral | Test | |
| Early | Late | p | ||
| N = 25 (%) | N = 175 (%) | |||
| Illiterate Elementaryschool Secondaryschool Highschool Universityand higher |
122 51 11 4 12 |
13(10.7) 9(17.6) 1(9.1) 2(50) 0(0) |
109(89.3) 42(82.4) 10(90.9) 2(50) 12(100) |
0.03* |
| χ2 Chi-squaretest *p = 0.03 is statistically significant. | ||||
The findings of this study show that the referral delay of cancer patients to the oncology unit in Armed Forces Hospitals Southern Regions can be attributed to patients, health facilities, and health professionals. It also showed that the patients believed that they were themselves the main cause of delay in their diagnosis of cancer, but also, they put some blame on health professionals for not educating them more and direct them on what to do after the first encountered visit. On the other hand, it was shown that health professionals were the first to be blamed as the main cause of the delay in the treatment of cancer, followed by the patients themselves as the second main cause, although there was no clinically meaningful delay in starting the treatment.
The results showed that the health professionals that the patients met at the beginning had a strong influence on their decision of accepting the treatment, confirming the major role of knowledgeable health professionals. Cancer knowledge is very important for patients to cope with their diagnosis and treatment, and might affect their survival. In one study involving breast and prostate cancer, the knowledge of the patients improved if the initial meeting time with the physician increase, and it was associated with improved patients’ anxiety [14].
Our study was also consistent with a study that showed a strong relationship between knowledge of self-examination of the breast and early diagnosis of breast cancer in Iranian women. [15]. A review article about cancer control in developing countries showed that low awareness of knowledge of risk factors, symptoms, or signs of cancer contribute to delays in early diagnosis and treatment. It further indicated that only a small proportion of the populations of developing countries have a decent knowledge of cancer [16]. Lack of knowledge and information is not only present in developing countries, but also, in less privileged populations in developed countries like some African American women, among whom breast cancer mortality was high. Poor information, beliefs, and fear of cancer were among the factors that contributed to delays in seeking health treatment [17]. One study conducted in Pakistan to assess the baseline knowledge of breast cancer revealed that 59% had poor knowledge of breast cancer [18]. Several other studies that have been reported in other developing countries showed similar results [19-21]
Seventy-five percent of our patients experienced delays in presentation longer than 2 months, which was associated with an advanced stage of cancer. This delay is worse than those presented in other studies conducted in developed and developing countries. The duration of delay in a study from the UK was 32% for more than 3 months [22], while a similar Iranian study revealed such delays in 23% [23]. However, our results were similar to those of a study from Malaysia, where 72.6% of patients experienced delays of more than 3 months and lack of knowledge contributed to this delay, as in our study [24].
Several studies have been conducted on patient delay in seeking treatment after diagnosis in many parts of the world. One large single-institution study of delay and survival from breast cancer in the UK showed that a longer duration of symptoms is associated with worse survival rates [22], and our study showed a clear association between delayed diagnosis and advanced disease. Age was not associated with delays in treatment or diagnosis in our study, and this was inconsistent among different trials [25,26].
This study demonstrated that 30% had used complementary and alternative medicine (CAM), contributing to delays in presentation, diagnosis, and seeking treatment. Most of the time, this involved advice from a relative or a person in the community. It was also found that local healers claimed that they have the power to cure patients, and around 80% of our patients believed them. This has been reported in a Malaysian study where the fear and lack of knowledge and advice from a relative influenced the use of CAM and led to a delay in diagnosis and management [27]. A few studies have investigated the prevalence of CAM use in Saudi Arabia, reporting values ranging from 20% to up to 90% [28-30].
Thirty percent of the study participants experienced delays because they were seeking treatment from tertiary hospitals. These findings imply that the patients had spent more time seeking treatment at tertiary hospitals outside the region, resulting in a delay in presentation.
Our data suggest that there is a definitive delay in the presentation of cancer patients living in the southern part of Saudi Arabia (level 1). Low educational level, poor knowledge of cancer symptoms, and use of complementary and alternative medicines are the main causes of delay. There were no meaningful clinical delays in diagnosis and start of treatment (level 2,3) indicating a good post-diagnosis health system.
People in the community, therefore, require education about the common presentations of different types of cancer.
Unfortunately, many people in our country still believe in CAM and local healers, and many still provide patients with incorrect advice.
We deeply thank our patients who agreed to participate in this study and all the staff in our hospitals who made great efforts to help us conduct it.
Statement of ethics: This study was approved by the local ethics committee, and informed consent was obtained from all participants.
Author contributions: All authors had contributed equally in planning, reviewing, and writing the paper.
- Hoyert DL, Xu J. Deaths: preliminary data for 2011. National Vital Statistics Reports. 2012; 61: 1-15.
- Saudi Cancer Registry. http://www.scr.org.sa/files/file/2010.pdf
- Almalki M, Fitzgerald G, Clark M. Health care system in Saudi Arabia: an overview. East Mediterr Health J. 2011; 17: 784-793. PubMed: https://pubmed.ncbi.nlm.nih.gov/22256414/
- Olaku O, Zia F, Santana JM, White JD. The National Cancer Institute best case series program: a summary of cases of cancer patients treated with unconventional therapies in India. Integr Cancer Ther. 2013; 12: 385-392. PubMed: https://pubmed.ncbi.nlm.nih.gov/23355475/
- Khalil RB. Attitudes, beliefs and perceptions regarding truth disclosure of cancer-related information in the Middle East: a review. Palliat Support Care. 2013; 11: 69-78. PubMed: https://pubmed.ncbi.nlm.nih.gov/23171758/
- Caswell G, Seymour J, Crosby V, Hussain A, Manderson C, et al. Lung cancer diagnosed following an emergency admission: exploring patient and carer perspectives on delay in seeking help. Support Care Cancer. 2017; 25: 2259-2266. PubMed: https://pubmed.ncbi.nlm.nih.gov/28220316/
- Tørring ML, Frydenberg M, Hansen RP, Olesen F, Vedsted P. Evidence of increasing mortality with longer diagnostic intervals for five common cancers: a cohort study in primary care. Eur J Cancer. 2013; 49: 2187-2198. PubMed: https://pubmed.ncbi.nlm.nih.gov/23453935/
- http://seer.cancer.gov/publications/uscs.html
- De Nooijer J, Lechner L, de Vries H. Help-seeking behaviour for cancer symptoms: perceptions of patients and general practitioners. Psychooncology. 2001; 478: 469-478. PubMed: https://pubmed.ncbi.nlm.nih.gov/11747059/
- Al-Rajhi N, El-Sebaie M, Khafaga Y, AlZahrani A, Mohamed G, et al. Nasopharyngeal carcinoma in Saudi Arabia: clinical presentation and diagnostic delay. East Mediterr Health J. 2009; 15: 1301-1307. PubMed: https://pubmed.ncbi.nlm.nih.gov/20214145/
- Hansen RP, Olesen F, Sørensen HT, Sokolowski I, Søndergaard J. Socioeconomic patient characteristics predict delay in cancer diagnosis: a Danish cohort study. BMC health services research. BMC Health Serv Res. 2008; 8: 49. PubMed: https://pubmed.ncbi.nlm.nih.gov/18307790/
- Sharma K, Costas A, Shulman LN, Meara JG. A Systematic Review of Barriers to Breast Cancer Care in Developing Countries Resulting in Delayed Patient Presentation. J Oncol. 2012; 2012: 121873. PubMed: https://pubmed.ncbi.nlm.nih.gov/22956949/
- Olesen F, Hansen RP, Vedsted P. Delay in diagnosis: the experience in Denmark. Br J Cancer. 2009; 101: 5–8. PubMed: https://pubmed.ncbi.nlm.nih.gov/19956163/
- Berger O, Grønberg BH, Loge JH, et al. Cancer patients’ knowledge about their disease and treatment before, during and after treatment: a prospective, longitudinal study. BMC Cancer. 2018; 18: 381. PubMed: https://pubmed.ncbi.nlm.nih.gov/29614997/
- Parsa P, Kandiah M. Breast cancer knowledge, perception and breast self-examination practices among Iranian women. Int Med J. 2005; 4: 17-24.
- Hanna P, Kangolle T. Cancer control in developing countries: using health data and health services research to measure and improve access, quality and efficiency. BMC Int Health Hum Rights. 2010; 10: 24. PubMed: https://pubmed.ncbi.nlm.nih.gov/20942937/
- Sadler GR, Ko CM, Cohn JA, White M, Weldon RN, et al. Breast cancer knowledge, attitudes, and screening behaviors among African American women: The Black cosmetologists promoting health program. BMC Public Health. 2007; 7: 57. PubMed: https://pubmed.ncbi.nlm.nih.gov/17439662/
- Khokher S, Qureshi W, Mahmood S, Saleem A, Mahmud S. Knowledge, attitude and preventive practices of women for breast cancer in the educational institutions of Lahore, Pakistan. Asian Pac J Cancer Prev. 2011; 12: 2419-2424. PubMed: https://pubmed.ncbi.nlm.nih.gov/22296394/
- Okobia MN, Bunker CH, Okonofua FE, Osime U. Knowledge, attitude and practice of Nigerian women towards breast cancer; a cross sectional study. World J Surg Oncol. 2006; 1: 4-11. PubMed: https://pubmed.ncbi.nlm.nih.gov/16504034/
- Rahman JA. Knowledge attitude and practice on breast cancer among female population of Alur Batu village, Kuantan and its related factors in June 2003. Singapore Med J0 2003; 10: 90-94.
- Ahmed BA. Awareness and practice of breast cancer and breast self examination among university students in Yemen. Asian Pac J Cancer Prev. 2010; 11: 101-105. PubMed: https://pubmed.ncbi.nlm.nih.gov/20593937/
- Richards MA, Smith P, Ramirez AJ, Fentiman IS, Rubens RD. The influence on survival of delay in the presentation and treatment of symptomatic breast cancer. Br J Cancer. 1999; 79: 858-864. PubMed: https://pubmed.ncbi.nlm.nih.gov/10070881/
- Montazeri A, Ebrahimi M, Mehrdad N, Ansari M, Sajadian A. Delayed presentation in breast cancer: a study in Iranian women. BMC Womens Health. 2003; 3: 4. PubMed: https://pubmed.ncbi.nlm.nih.gov/12846932/
- Norsa'adah B, Rampal KG, Rahmah MA, Naing NN, Biswal BM. Diagnosis delay of breast cancer and its associated factors in Malaysian women. BMC Cancer. 2011; 11: 141. PubMed: https://pubmed.ncbi.nlm.nih.gov/21496310/
- Afzelius P, Zedeler K, Sommer H, Mouridsen HT, Blichert-Toft M. Patient’s and doctor’s delay in primary breast cancer. Acta Oncol. 1994; 33: 345-351. PubMed: https://pubmed.ncbi.nlm.nih.gov/8018364/
- Machiavelli M, Leone B, Romero A, Perez J, Vallejo C, et al. Relation between delay and survival in 596 patients with breast cancer. Oncology. 1989; 46: 78-82. PubMed: https://pubmed.ncbi.nlm.nih.gov/2710480/
- Mohd Mujar NM, Dahlui M, Emran NA, Abdul Hadi I, Wai YY, et al. Complementary and alternative medicine (CAM) use and delays in presentation and diagnosis of breast cancer patients in public hospitals in Malaysia. PLoS ONE. 2017; 12: e0176394. PubMed: https://pubmed.ncbi.nlm.nih.gov/28448541/
- Sait KH, Anfinan NM, Eldeek B, Al-Ahmadi J, Al-Attas M, et al. Perception of patients with cancer towards support management services and use of complementary alternative medicine.. A single institution hospital-based study in Saudi Arabia. Asian Pac J Cancer Prev. 2014; 15: 2547-2554. PubMed: https://pubmed.ncbi.nlm.nih.gov/24761862/
- Jazieh AR, Al Sudairy R, Abulkhair O, Alaskar A, Al Safi F, et al. Use of complementary and alternative medicine by patients with cancer in Saudi Arabia. J Altern Complement Med. 2012; 18: 1045-1049. PubMed: https://pubmed.ncbi.nlm.nih.gov/22906212/
- Abuelgasim KA, Alsharhan Y, Alenzi T, Alhazzani A, Ali YZ, et al. The use of complementary and alternative medicine by patients with cancer: a cross-sectional survey in Saudi Arabia. BMC Complement Altern Med. 2018; 18: 88. PubMed: https://pubmed.ncbi.nlm.nih.gov/29530034/