
More Information
Submitted: December 29, 2021 | Approved: March 28, 2022 | Published: March 29, 2022
How to cite this article: Utami AT, Wahidmurni, Walid M. The effects of religiosity and knowledge on the perceptions and attitude of muslim doctors that influence the intentions that impact on behavior in using halal drugs in Indonesia. J Community Med Health Solut. 2022; 3: 021-026.
DOI: 10.29328/journal.jcmhs.1001016
Copyright License: © 2022 Utami AT, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Religiosity; Knowledge; Perception; Attitude; Intention; Behavior; Halal medicine; Indonesia

The effects of religiosity and knowledge on the perceptions and attitude of muslim doctors that influence the intentions that impact on behavior in using halal drugs in Indonesia
Amalia Tri Utami1* Wahidmurni2 and Muhammad Walid2
1Faculty of Medicine and Health Science, Maulana Malik Ibrahim State Islamic University, Indonesia
2Faculty of Tarbiyah and Teaching Training, Maulana Malik Ibrahim State Islamic University, Indonesia
*Address for Correspondence: Amalia Tri Utami, Faculty of Medicine and Health Science, Maulana Malik Ibrahim State Islamic University, Indonesia, Email: [email protected]
Introduction: In the spirit of maintaining health and seeking medicine to cure a disease, the question of halal and haram still needs to be answered. This coincides with the words of the Prophet Muhammad SAW “Verily Allah does not make your healing in what He has forbidden you” (HR. Imam Bukhari). The purpose of this quantitative study was to determine the effect of religiosity, perception, knowledge, and attitudes of Muslim doctors on the use of halal drugs in Indonesia.
Materials and methods: This quantitative research method with correlational type examines the relationship between religiosity, perceptions, knowledge, attitudes, intentions, and behaviors that are shared online using google form. Data was measured using a Likert scale. A five-point Likert scale was used for statements: Strongly Disagree: 1, Disagree: 2, Uncertain: 3, Agree: 4, and Strongly Agree: 5. The sample size used was 435 Muslim doctors. The data obtained were then processed using the SmartPLS 3.0 application.
Results: The results obtained are that there is a relationship between the religiosity of Muslim doctors on perceptions so as to encourage intention so that there is a change in behavior in the use of halal drugs in Indonesia. In addition, there is a relationship between knowledge and attitudes so as to encourage intentions that cause behavioral changes in the use of halal drugs in Indonesia by Muslim doctors. In fact, every practice depends on the intention, therefore it is important to maintain the intention, which in this study is influenced by perceptions and attitudes so that charity will result in commendable behavior that is blessed by Allah SWT. In addition, there is also a need for education about halal drugs that are appropriate to be taught at the medical faculty of Islamic universities in Indonesia.
Religion is an interesting topic for researchers and practitioners of social scientists who want to uncover consumption habits, well-being, and the life of a person in general [1]. Religiosity as a measure of the extent to which people hold and practice beliefs in certain religious values and ideas has been used to operationalize religious constructions [2-5].
Researchers examined aspects of the religiosity and knowledge of Muslim doctors, because very interested to understand how religiosity and knowledge can affect a person’s desire to change the use of doctors of conventional medicine to be halal because most of them consider the wishes and lawful drug procurement to determine the quality of life [6-10].
However, in the enthusiasm for maintaining a healthy body and finding a cure for a disease, the question of halal and haram still needs to be addressed. Finding and choosing halal medicine is a must for all Muslims. Staying away from haram is also a human responsibility. This coincides with the words of the Prophet SAW “Seeking halal is obligatory for every Muslim” (HR.Ibnu Qudamah) [11].
This was a quantitative research method with a correlational type that examines the relationship between religiosity, perceptions, knowledge, attitudes, intentions, and behaviors that are shared online using Google Forms. Data was measured using a Likert scale. A five-point Likert scale was used for statements: Strongly Disagree: 1, Disagree: 2, Uncertain: 3, Agree: 4, and Strongly Agree: 5. The sample size used was 435 Muslim doctors. The data obtained were then processed using the SmartPLS 3.0 application.
The general description of the respondents is all Muslim doctors who are registered with the Indonesian KKI and are willing to fill out questionnaires that have been distributed on dr.amaliatriutami’s Instagram and several telegram groups. specifically for doctors throughout the territory of the Republic of Indonesia. Then from the respondents, the demographic description of respondents based on gender is described in Graph 1. Which is male respondents are 257 and female respondents are 178. So the total of respondents is 435 Muslim doctors.
Graph 1: Distribution of Respondents by Gender.
And from the distribution of the age, we found that 96.8% of respondents are 20-50 years old, only 3.2% are above 50 years old. And for the location where the respondents work are the clinic (38.8%), Independence practice (37.5%), and hospital (23,7%) (Graph 2).
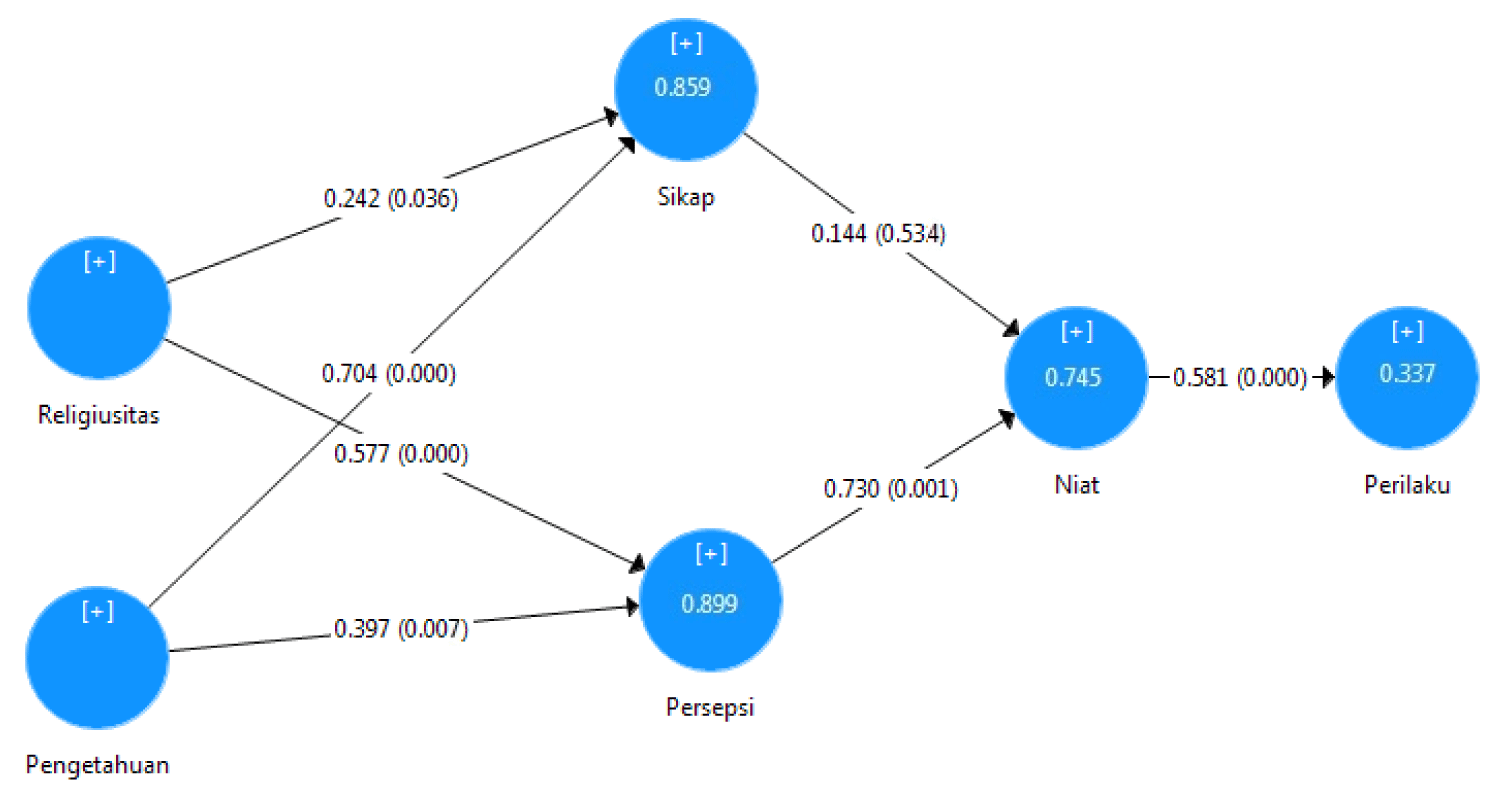
Graph 2: Path Analysis for Output Result.
For hypothesis testing, it can be seen from the probability value and the t-statistics value. The statistical value used is 5% alpha so the t - statistic value is 1.96. So the acceptance criteria if Ha is accepted and Ho is rejected when t - statistics > 1.96. To reject or accept the hypothesis using probability then Ha is accepted if the p - value < 0.05. Based on the empirical data used in this study, it is possible to test the hypothesis through path coefficients and t - statistics, and p - value.
a) Direct effect of exogenous variables on endogenous variables
This direct effect shows the direct effect of exogenous variables on endogenous variables without involving mediating variables. The results of hypothesis testing are presented as follows:
H1: Religiosity (W1) affects the attitude of Muslim doctors (X1)
The estimation results of the inner model for the direct influence of religiosity on attitudes show a p - value (p - value) of 0.036, where the value is smaller than alpha 0.05, so it can be concluded that there is a (direct effect) which is positively significant between religiosity on attitudes of 0.242. The positive influence of religiosity on attitudes can be interpreted that the higher the religiosity, the higher the attitude. On the other hand, the lower the religiosity, the lower the attitude. These results indicate that the hypothesis is accepted.
H1: Religiosity (W1) affects the perception of Muslim doctors (X2)
The estimation results of the inner model for the direct influence of religiosity on perception show a p - value (p - value) of 0.000, where the value is smaller than alpha 0.05, so it can be concluded that there is the (direct effect) which is positively significant between religiosity on perception is 0.577. The positive effect of religiosity on perception can be interpreted that the higher the religiosity, the higher the perception. On the other hand, the lower the religiosity, the lower the perception. These results indicate that the hypothesis is accepted.
H1: Knowledge (W2) affects the Attitude of Muslim Doctors (X1)
The estimation results of the inner model for the direct effect of knowledge on attitudes show a p - value (p - value) of 0.000, where the value is smaller than alpha 0.05, so it can be concluded that there is the (direct effect) which is positively significant between knowledge and attitude is 0.704. The positive effect of knowledge on attitudes can be interpreted that the higher the knowledge, the higher the attitude. On the other hand, the lower the knowledge, the lower the attitude. These results indicate that the hypothesis is accepted.
H1: Knowledge (W2) affects the perception of Muslim doctors (X2)
The estimation results of the inner model for the direct effect of knowledge on perception show a p - value (p - value) of 0.007, where the value is smaller than alpha 0.05, so it can be concluded that there is a (direct effect) which is positively significant between knowledge and perception is 0.397. The positive effect of knowledge on perception can be interpreted that the higher the knowledge, the higher the perception. On the other hand, the lower the knowledge, the lower the perception. These results indicate that the hypothesis is accepted.
H1: Muslim Doctor’s Attitude (X1) has an effect on Intention (Y1)
The estimation results of the inner model for the direct effect of attitude on intention show a p - value (p - value) of 0.034, where the value is smaller than alpha 0.05, so it can be concluded that there is a significant direct effect between attitudes towards intentions. In other words, the influence between attitudes towards intentions is 0.644, so high or low attitudes affect the level of intention. These results indicate that the hypothesis is accepted.
H1: Perception of Muslim Doctors (X2) has an effect on Intention (Y1)
The estimation results of the inner model for a direct influence between perception on intention show a p - value (p - value) of 0.001, where the value is smaller than alpha 0.05, so it can be concluded that there is a (direct effect) which is positively significant between perceptions of intentions is 0.730. The positive effect of perception on intention can be interpreted that the higher the perception, the higher the intention. On the other hand, the lower the perception, the lower the intention. These results indicate that the hypothesis is accepted.
H1: Intention (Y1) has an effect on behavior (Z1)
The estimation results of the inner model for the direct effect of intention on behavior show a p - value (p - value) of 0.000, where the value is smaller than alpha 0.05, so it can be concluded that there is a direct influence (direct effect) which is positively significant between intention and behavior is 0.581. The positive influence of intention on behavior can be interpreted that the higher the intention, the higher the behavior. On the other hand, the lower the intention, the lower the behavior. These results indicate that the hypothesis is accepted.
b) Indirect effect of exogenous variables on endogenous variables
It shows the magnitude of the direct effect of exogenous variables on endogenous variables by involving mediating variables.
H1: Religiosity (W1) has an indirect effect on Muslim Doctors’ Intentions (Y1) through Attitude (X1)
Path coefficient value for indirect influence between religiosity through the attitude towards the intention of 0.035 shows a p - value of 0.608 which is greater than 0.05, so it can be concluded that the indirect effect between religiosity through attitude towards intention is not significant. In other words, high or low religiosity has no significant effect on increasing or decreasing attitudes, it will also have no effect on increasing or decreasing intentions. The hypothesis is rejected.
H1: Religiosity (W1) has an indirect effect on Muslim Doctors’ Intentions (Y1) through Perception (X2)
The path coefficient value for an indirect effect between religiosity through the perception of the intention of 0.421 shows a p - value of 0.003 which is smaller than 0.05, so it can be concluded that the indirect effect between religiosity through the perception of intention is significant. In other words, the higher the religiosity, it will affect the increase in perception, so that the increase in perception will increase the intention. On the other hand, the lower the religiosity, the lower the perception will be, so that the lower the perception will lower the intention. The hypothesis is accepted.
H1: Knowledge (W2) has an indirect effect on Muslim Doctors’ Intentions (Y1) through Attitude (X1)
The path coefficient value for the indirect effect between knowledge through attitudes towards intentions is 0.401, indicating a p - value of 0.048 which is smaller than 0.05, so it can be concluded that the indirect effect of knowledge through attitudes on intentions is significant. In other words, high or low knowledge has a significant effect on increasing or decreasing attitudes, this will also have an effect on increasing or decreasing intentions. The hypothesis is accepted.
H1: Knowledge (W2) has an indirect effect on Muslim Doctors’ Intentions (Y1) through Perception (X2)
The path coefficient value for the indirect effect between knowledge through the perception of the intention of 0.289 shows a p - value of 0.080 which is greater than 0.05, so it can be concluded that the indirect effect of knowledge through the perception of intention is not significant. In other words, high or low knowledge has no significant effect on increasing or decreasing perception, it will also have no effect on increasing or decreasing intention. The hypothesis is rejected.
H1: Attitude (X1) has an indirect effect on the behavior of Muslim doctors (Z1) through intentions (Y1)
The path coefficient value for the indirect effect between attitudes through intention to the behavior of 0.084 shows a p - value of 0.546 which is greater than 0.05, so it can be concluded that the indirect effect between attitudes through intention to behavior is not significant. In other words, the high or low attitude has no significant effect on increasing or decreasing intention, it will also have no effect on increasing or decreasing behavior. The hypothesis is rejected.
H1: Perception (X2) has an indirect effect on the behavior of Muslim doctors (Z1) through Intention (Y1).
The path coefficient value for the indirect effect between Perception through intention on behavior is 0.424, indicating a p - value of 0.001 which is smaller than 0.05, so it can be concluded that the indirect effect of perception through intention on behavior is significant. In other words, the higher the perception, it will affect the increase in intention, so that the increase in intention will increase behavior. On the other hand, the lower the perception, the lower the intention, so that the lower the intention will also reduce the behavior. The hypothesis is accepted.
H1: Religiosity (W1) has an indirect effect on Behavior (Z1) through Attitude (X1) and Intentions of Muslim Doctors (Y1)
Path coefficient value for indirect influence between religiosity through attitudes and intentions towards the behavior of 0.020 shows a p - value of 0.615 which is greater than 0.05, so it can be concluded that the indirect effect between religiosity through attitudes and intentions towards behavior is not significant. In other words, high or low religiosity has no significant effect on increasing or decreasing attitudes and intentions, it will also have no effect on increasing or decreasing behavior. The hypothesis is accepted.
H1: Religiosity (W1) has an indirect effect on Behavior (Z1) through Perception (X2) and Intentions of Muslim Doctors (Y1).
The path coefficient value for the indirect influence between religiosity through perception and intention on behavior is 0.244, indicating a p - value of 0.003 which means smaller than 0.05, so it can be concluded that the indirect effect of religiosity through perceptions and intentions on behavior is significant. In other words, the higher the religiosity, it will have an effect on increasing perceptions and intentions, so that with increased perceptions and intentions it will increase behavior. On the other hand, the lower the religiosity, the lower the perception and intention, so that the lower the perception and intention will reduce the behavior. The hypothesis is accepted.
H1: Knowledge (W2) has an indirect effect on Behavior (Z1) through Attitude (X1) and Intentions of Muslim Doctors (Y1)
Path coefficient value for indirect influence between knowledge through attitude and intention to the behavior of 0.059 indicates a p - value of 0.564 which is greater than 0.05, so it can be concluded that the indirect influence between knowledge through attitude and intention to behavior is not significant. In other words, high or low knowledge has no significant effect on increasing or decreasing attitudes and intentions, it will also have no effect on increasing or decreasing behavior. The hypothesis is rejected.
H1: Knowledge (W2) has an indirect effect on Behavior (Z1) through Perception (X2) and Intentions of Muslim Doctors (Y1)
The path coefficient value for the indirect effect between knowledge through perception and intention on behavior is 0.168 indicating a p - value of 0.089 which is greater than 0.05, so it can be concluded that the indirect effect between knowledge through perception and intention on behavior is not significant. In other words, high or low knowledge has no significant effect on increasing or decreasing perceptions and intentions, it will also have no effect on increasing or decreasing behavior. The hypothesis is rejected.
This study was conducted to evaluate aspects of religiosity, knowledge, attitudes, perceptions, and intentions of Muslim doctors regarding the behavior of using halal drugs in Indonesia. The previous intensive literature review found no studies of this kind carried out on issues surrounding Halal medicines among the general public. Medicines have become a necessity now to maintain health. There are usually three important players in this context, doctors, pharmacists, and consumers.
Patients usually cannot judge which drug is right for them. This is then the role of Muslim doctors to choose the most suitable drug for their patients by keeping in mind the patient’s religious beliefs. An important aspect of consideration when prescribing a drug regimen is the aspect of religiosity. Each individual has a different view of treatment, including the use of certain inactive ingredients in medicines.
Muslim doctors and pharmacists should be proactive and not leave the patient to start the conversation. Since patients have the right to make informed decisions about their medical care, health care providers must involve patients when making treatment decisions. The current study finds positive perceptions about halal medicines.
As in Indonesia, the development of the halal drug industry is important because the largest Muslim population in the world is in Indonesia. It is also necessary to understand the factors that influence changes in the behavior of Muslim doctors to use halal medicinal products. Therefore, this study was successful in investigating important issues related to the behavior of Muslim doctors in Indonesia. By using the TPB framework that combines religiosity and knowledge of halal drugs in addition to the original TPB variables, this study found a positive effect of religiosity and knowledge on perceptions and attitudes to encourage intention and ultimately change in behavior of using halal drugs.
Apart from the above results, this study has some limitations. In terms of models, it is recognized that the current TPB model is limited in its capacity to explain the intention to consume halal medicinal products in Indonesia. Therefore, future studies may expand the model to include more explanatory variables (such as safety, health awareness, past behavior, beliefs, value prices, and income) or more items in each variable (such as the inclusion of physician influence in subjective norm variables). It is also possible to investigate the moderating and mediating effects of the variables on customer intentions and use other methods, such as experimental methods and sentiment analysis, to investigate this issue slightly differently.
In terms of the sample, although the google form has been distributed to the population representing almost all the major ethnic groups in the country, the results discussed above may have limited generalizability and should be interpreted with caution. In this regard, it is suggested that further research should broaden the scope of the research to capture more diversity in market conditions, geography, and demographics. It is also possible to scale studies to reach more specific targets/areas (such as urban, rural, and across gender) and other countries. This additional aspect will provide more insight into consumer behavioral intentions in consuming halal medicinal products.
Research-based halal drug education curricula need to be continuously developed in the education of medical faculties at Islamic universities in Indonesia, as well as the world in the future. This is important to instill a caring attitude about Islamic law which is quite crucial in the field of medicine today. Answering problems related to halal and haram in the use of drugs can be the first step in providing competent and rational health services.
Muslim doctors who are deeply religious will evaluate the world through religious schemes and will thus integrate their religion into most of their lives. If followers are very receptive to their religious doctrines, they tend to adhere to the rules and ethical codes set by their religious doctrine, for example only eating halal products, attending worship regularly on holy days, and strictly practicing religious practices and group membership. On the other hand, if their belief in religious teachings is weak, they may feel free to behave in other ways. Therefore, increasing Islamic values in the form of Islamic religious lessons needs to be taught, especially at the university level. This study has a weakness because it uses an online method because of the restricted activity during the COVID-19 era, allowing for population bias when filling out.
Religiosity appears to impact Muslim physician attitudes toward various aspects of end-of-life healthcare decision-making.11Religious beliefs and values impact Muslim patients’ attitudes toward a variety of healthcare decisions, including organ donation. Muslim physician attitudes toward organ donation, however, are less well studied. Utilizing a national survey of physician members of the Islamic Medical Association of North America, relationships between religiosity, patterns of bioethics resource utilization, and sociodemographic characteristics with attitudes toward organ donation were assessed. Several socio-demographic features had a positive association with believing organ donation to be permitted: ethnic descent other than that of South Asian, having immigrated to the USA as an adult, and male sex. When using a logistic regression model controlling for these three variables as potential confounders, the best predictor of Muslim physicians believing organ donation to be permissible was the utilization of an Imam as a bioethical resource (odds ratio 5.9, p = 0.02). Religiosity variables were not found to be associated with views on the Islamic permissibility of organ donation. While Muslim American physicians appear to believe there is religious support for organ donation, only a minority sign up to be donors. A greater study is needed to understand how physicians’ attitudes regarding donation impact discussions between patients and physicians regarding the possibility of donating and of receiving a transplant [12].
This study is an opportunity for Muslim doctors about the potential for religiosity and knowledge to open the spirit of Muslim doctors in making new procedures related to the management of existing diseases using halal medicinal preparations. Because it does not deny that the medicines used as therapeutic management that are oriented to WHO use drugs that are not clearly halal so that they are not appropriate when used as guidelines, because Muslims have a grip in the form of the Qur’an and Sunnah.
The results obtained are that there is a relationship between the religiosity of Muslim doctors on perceptions so as to encourage intention so that there is a change in behavior in the use of halal drugs in Indonesia. In addition, there is a relationship between knowledge and attitudes so as to encourage intentions that cause behavioral changes in the use of halal drugs in Indonesia by Muslim doctors. In fact, every practice depends on the intention, therefore it is important to maintain the intention, which in this study is influenced by perceptions and attitudes so that charity will result in commendable behavior that is blessed by Allah SWT. In addition, there is also a need for education about halal drugs that are appropriate to be taught at the medical faculty of Islamic universities in Indonesia.
- Rakrachakarn V, Moschis GP, Ong FS, Shannon R. Materialism and life satisfaction: the role of religion. J Relig Health. 2015; 54: 413-426. PubMed: https://pubmed.ncbi.nlm.nih.gov/24233840/
- Singhapakdi A, Vitell SJ, Lee DJ, Nisius AM, Yu GB. The inflfluence of love of money and religiosity on ethical decision-making in marketing. J Business Ethics. 2012; 114: 183-191.
- Bakar A, Lee R, Hazarina Hashim N. Parsing religiosity, guilt and materialism on consumer ethics. J Islamic Marketing. 2013; 4: 232-244.
- Karami M, Olfati O, Dubinsky A. Influence of religiosity on retail salespeople’s ethical perceptions: the case in Iran. J Islamic Marketing. 2013; 5: 144-172.
- Pace S. Effects of intrinsic and extrinsic religiosity on attitudes toward products: empirical evidence of value-expressive and social-adjustive functions. J Appl Busin Res. 2014; 30:1227-1238.
- Rakrachakarn V, Moschis GP, Ong FS, Shannon R. Materialism and life satisfaction: the role of religion. J Relig Health. 2015; 54: 413-426. PubMed: https://pubmed.ncbi.nlm.nih.gov/24233840/
- Yousaf S, Shaukat Malik M. Evaluating the inflfluences of religiosity and product involvement level on the consumers. J Islamic Marketing. 2013; 4: 163-186.
- Singhapakdi A, Vitell SJ, Lee DJ, Nisius AM, Yu GB. The inflfluence of love of money and religiosity on ethical decision-making in marketing. J Business Ethics. 2012; 114: 183-191.
- Bakar A, Lee R, Hazarina Hashim N. Parsing religiosity, guilt and materialism on consumer ethics. J Islamic Marketing. 2013; 232-244.
- Vitell SJ, Bing MN, Davison HK, Ammeter AP, Garner BL, et al. Religiosity and moral identity: the mediating role of self-control. J Business Ethics. 2008; 88: 601-613.
- Duivenbode R, Hall S, Padela AI. Assessing relationships between muslim physicians' religiosity and end-of-life health-care attitudes and treatment recommendations: an exploratory national survey. Am J Hosp Palliat Care. 2019; 36: 780-788. PubMed: https://pubmed.ncbi.nlm.nih.gov/30813738/
- Ahmed M, Kubilis P, Padela A. American Muslim Physician Attitudes Toward Organ Donation. J Relig Health. 2018; 57: 1717-1730. PubMed: https://pubmed.ncbi.nlm.nih.gov/30076496/