
More Information
Submitted: May 11, 2026 | Accepted: May 25, 2026 | Published: May 26, 2026
Citation: Akhssas A, Belahrach A, Ouhrich I, Bennamara FZ, Belahrach A, Najib M, et al. Rhinovirus and Acute Respiratory Infections in Hospitalized Children a Moroccan Retrospective Study 2021–2025. J Community Med Health Solut. 2026; 7(1): 59-65. Available from:
https://dx.doi.org/10.29328/journal.jcmhs.1001074
DOI: 10.29328/journal.jcmhs.1001074
Copyright license: © 2026 Akhssas A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Rhinovirus; Multiplex PCR; Acute respiratory infections; Pediatrics; Film array; Morocco

Rhinovirus and Acute Respiratory Infections in Hospitalized Children a Moroccan Retrospective Study 2021–2025
A Akhssas1 , A Belahrach1, I Ouhrich1, FZ Bennamara1, A Belahrach1, M Najib1, H Azzouzi1, N Mchichou1, Z Bouassaba1, E Bouaiti1, MR Tagajdid1, H Elannaz1, S Hassine1, S Ouannass1, A Reggad1, M Elqatni1, Z Kasmi1, A Laraqui1, N Touil1, B Machichi1, A Radi2, A Ourrai2, R Abilkassem2, M Elouennass1, K Ennibi1, R Abi1* and I Lahlou Amine1
, A Belahrach1, I Ouhrich1, FZ Bennamara1, A Belahrach1, M Najib1, H Azzouzi1, N Mchichou1, Z Bouassaba1, E Bouaiti1, MR Tagajdid1, H Elannaz1, S Hassine1, S Ouannass1, A Reggad1, M Elqatni1, Z Kasmi1, A Laraqui1, N Touil1, B Machichi1, A Radi2, A Ourrai2, R Abilkassem2, M Elouennass1, K Ennibi1, R Abi1* and I Lahlou Amine1
1Virology Laboratory, Biomedical and Epidemiology Research Unit (URBE), Centre of Virology, Infectious and Tropical Diseases (CVMIT), Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco
2Department of Pediatrics, Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco
*Corresponding author: Rachid Abi, Virology Laboratory, Biomedical and Epidemiology Research Unit (URBE), Centre of Virology, Infectious and Tropical Diseases (CVMIT), Mohammed V Military Teaching Hospital, Mohammed V University, Rabat, Morocco, Email: [email protected]
Background: Acute respiratory infections (ARI) remain a leading cause of morbidity and mortality in children under five. Multiplex PCR enables rapid identification of a wide range of respiratory pathogens. This study assessed the role of Rhinovirus in pediatric ARI in Morocco.
Methods: A retrospective descriptive study was conducted at the Virology Laboratory of Mohammed V Military Teaching Hospital (HMIMV) in Rabat, from September 2021 to September 2025, including 125 children under five years of age hospitalized in pediatrics and tested with the FilmArray Respiratory Panel (BioFire®).
Results: The mean age was 3 years, with a male predominance (M/F sex-ratio = 1.36). The PCR positivity rate was 72.0% (n = 90). A total of 122 pathogens were identified (118 viral, 4 bacterial). Rhinovirus/Enterovirus was the most frequent agent (42.4%), followed by RSV (15.3%), SARS-CoV-2 (11.9%), and Adenovirus (10.2%). Co-infections accounted for 35.6% of positive samples, mostly virus–virus.
Conclusion: Multiplex respiratory PCR confirms the leading role of Rhinovirus in pediatric ARI in Morocco in the post-COVID era and represents a key tool for diagnostic and therapeutic guidance.
In Morocco, acute respiratory infections (ARI) are the leading reason for antibiotic prescription and represent a major public health concern in the pediatric population. They remain the leading cause of morbidity and mortality in children under five in developing countries [1]. In Morocco, ARI accounts for approximately 25 to 30% of hospital admissions in children under five [2].
Molecular biology has revolutionized the management of ARI in both adults and children. The low sensitivity of conventional methods, the high frequency of viruses among causative pathogens, and the very short turnaround time of current molecular techniques — particularly multiplex PCR — have made this technique a powerful solution for improved diagnostic and therapeutic management of ARI [3].
Among the infectious agents causing pediatric ARI, the respiratory syncytial virus (RSV) has classically been considered the primary cause of bronchiolitis. In recent years, however, Rhinovirus has emerged with increasing prominence among agents associated with pediatric ARI.
This study, conducted at the Virology Laboratory of Mohammed V Military Teaching Hospital (HMIMV) in Rabat, aimed to evaluate the contribution of multiplex PCR in the etiological diagnosis of Rhinovirus-related respiratory infections in a pediatric ward.
Study design, setting, and period
This was a retrospective descriptive study conducted at the Virology Laboratory of Mohammed V Military Teaching Hospital in Rabat. The study included all respiratory multiplex PCR tests performed in children hospitalized in the pediatric ward over four years, from September 2021 to September 2025.
Inclusion and exclusion criteria
Inclusion criteria were:
- Children hospitalized in the pediatric ward of HMIMV.
- Age below five years at the time of admission.
- Multiplex PCR was performed on a respiratory specimen in the presence of suggestive respiratory symptoms.
Exclusion criteria were:
- Age above five years.
- Hospitalization in a ward other than pediatrics.
- Outpatient management only, without hospitalization.
Data collection
Data was extracted from the laboratory information system of the virology laboratory using the DX Lab software. The variables collected included age, sex, year of sampling, multiplex PCR result, type and name of identified pathogens, and available biological parameters, particularly C-reactive protein (CRP) and leukocyte count.
Specimens and microbiological analysis
Respiratory specimens were obtained by nasopharyngeal and/or oropharyngeal swabbing, with nasopharyngeal sampling preferred whenever possible. Samples were analyzed using the Film Array Respiratory Panel (BioFire®), which enables simultaneous detection of 16 viruses and 4 respiratory bacteria. The system automatically performs sample preparation, nucleic acid extraction, nested multiplex PCR, and target detection [4].
It should be noted that the Film Array panel does not differentiate Rhinovirus from Enterovirus, as these two viruses — both belonging to the Picornaviridae family — are jointly detected within a single target.
Demographic characteristics
A total of 125 hospitalized children who underwent respiratory multiplex PCR were included. Age ranged from 1 month to 5 years, with a mean of 3 years. The 3–4 years age group was the most represented, with 80 patients (64.0%) (Figure 1).

Figure 1: Distribution of patients by age group (n = 125).
The population comprised 72 boys (57.6%) and 53 girls (42.4%), with an M/F sex-ratio of 1.36 (Figure 2).
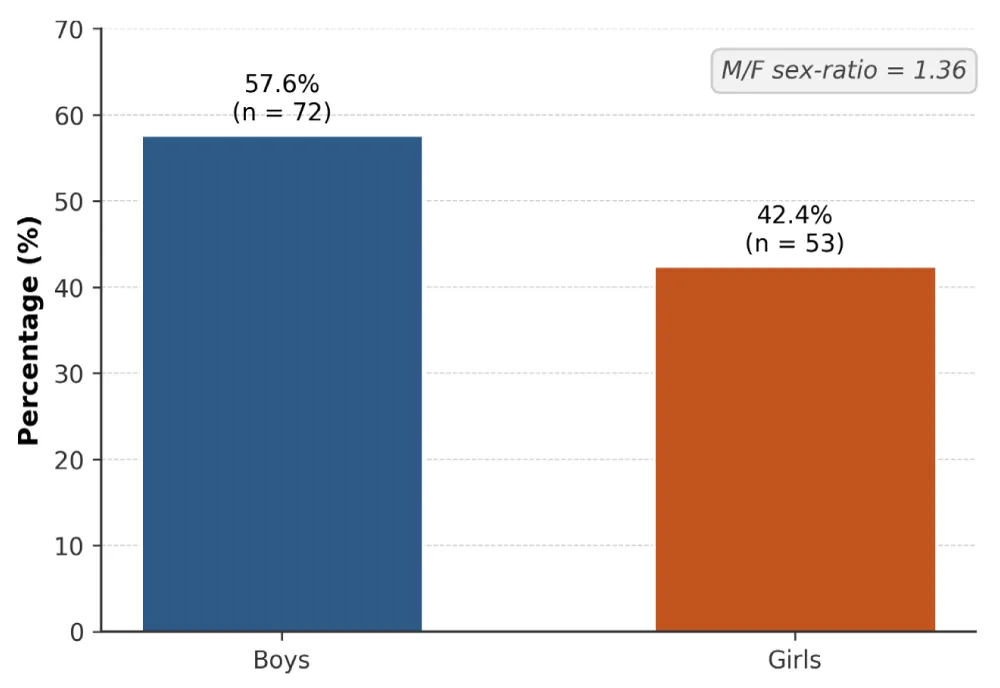
Figure 2: Distribution of patients by sex (n = 125).
Yearly distribution of samples
The yearly distribution of samples (Figure 3) showed a clear concentration of cases during the 2022/2023 season (61.6%).
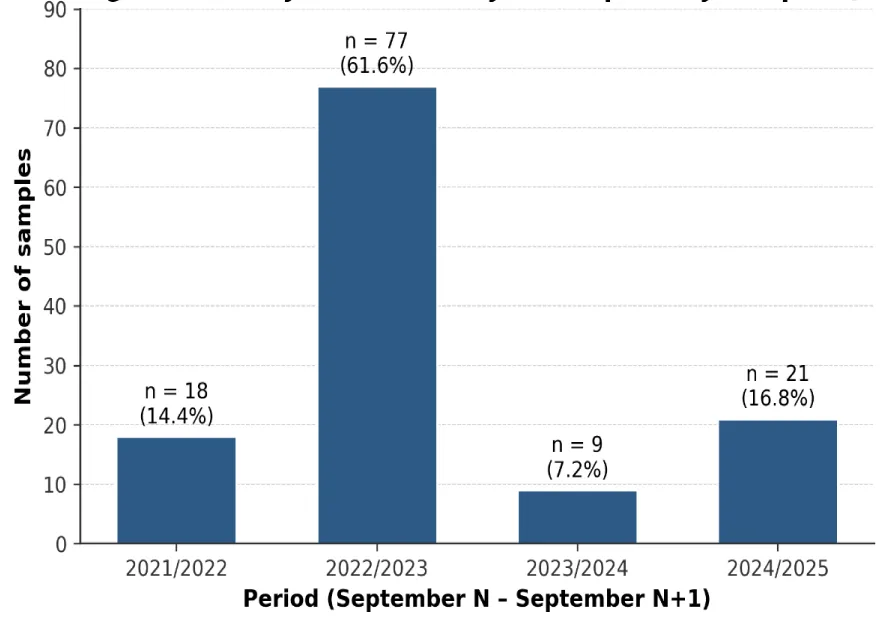
Figure 3: Yearly trend of analyzed respiratory samples (n = 125).
Biological parameters
CRP analysis in the 125 children showed that nearly half of the patients had a normal CRP (47.2%). Mild and moderate elevations were observed in 19.2% and 23.2% of cases, respectively, while very high CRP (> 100 mg/L) concerned 10.4% of patients (Figure 4).
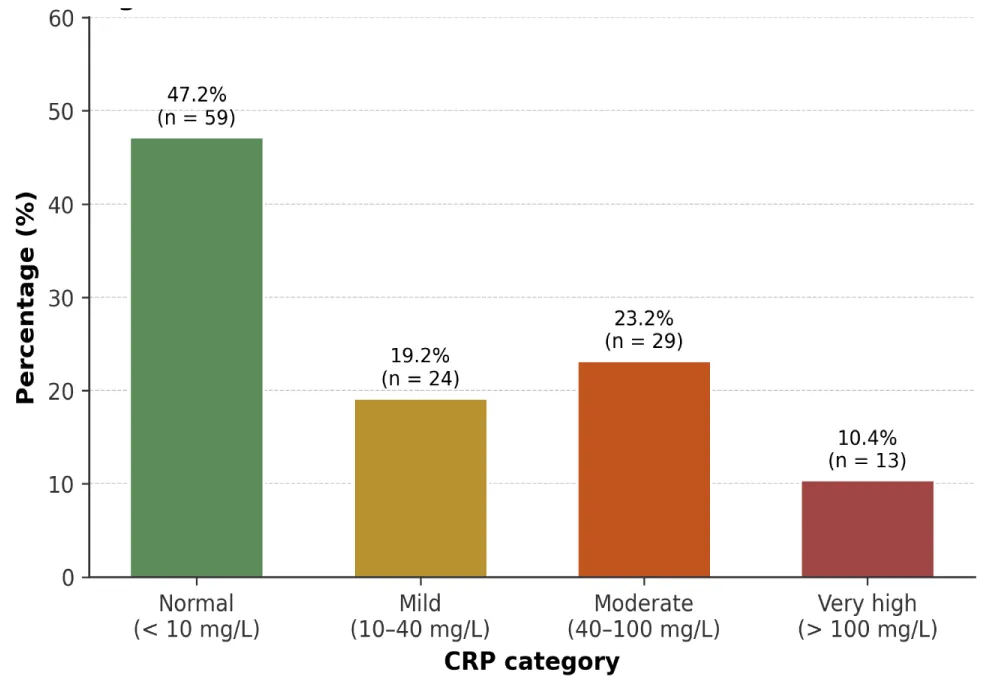
Figure 4: Distribution of CRP values (n = 125).
Interpretation of the leukocyte count, taking into account the physiological reference values specific to each pediatric age range, showed that most patients had a normal leukocyte count (68.0%). Moderate leukocytosis was observed in nearly one-third of cases (29.6%), while marked leukocytosis remained rare (2.4%) (Figure 5).
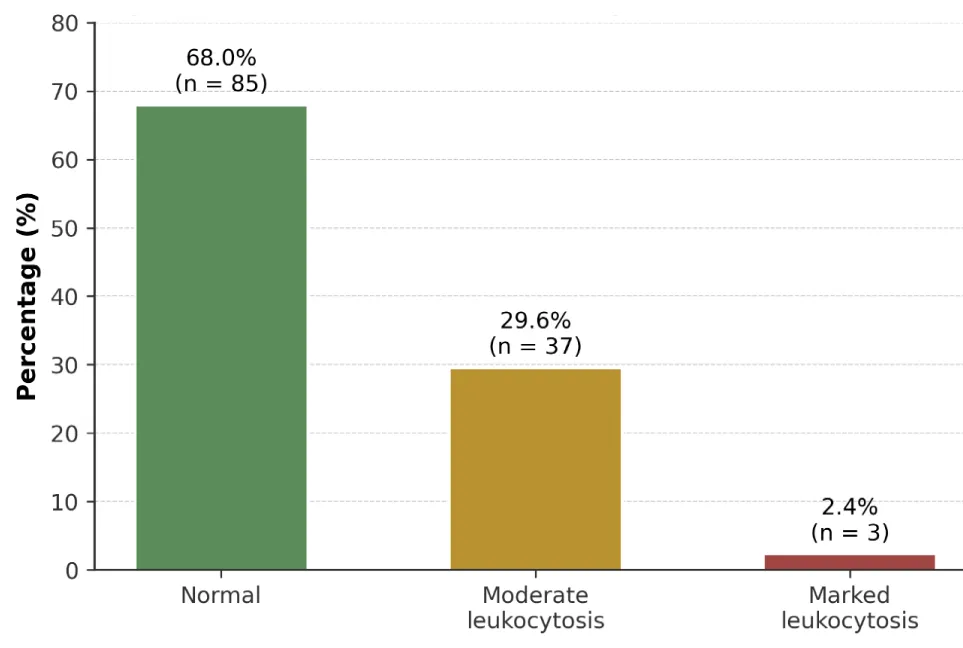
Figure 5: Distribution of leukocyte count (n = 125).
Multiplex PCR results
Of the 125 samples analyzed, 90 were positive (72.0%), 32 were negative (25.6%), and 3 could not be performed (2.4%), reflecting a majority of positive tests (Figure 6).
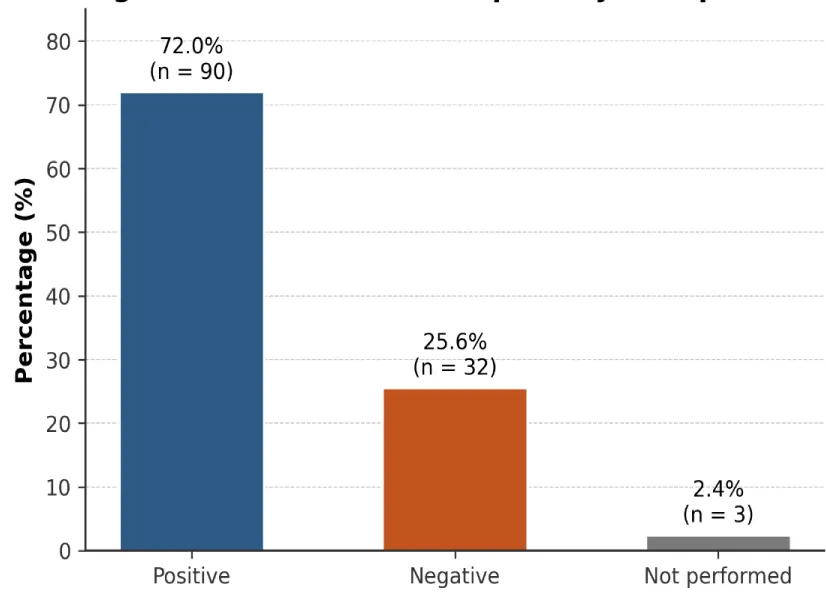
Figure 6: Results of the respiratory multiplex PCR (n = 125).
Identified pathogens
Although 90 samples were classified as positive, a total of 122 pathogens were identified. This discrepancy is explained by the simultaneous detection of several infectious agents within a single sample, reflecting the presence of co-infections. Overall, 16 distinct organisms were identified, including 13 viral species and 3 bacterial species (Table 1).
| Table 1: Total number of pathogens identified. | ||
| Category | Detections (n) | Number of species |
| Viruses | 118 | 13 |
| Bacteria | 4 | 3 |
| Total | 122 | 16 |
The 118 viral detections were distributed as follows: Rhinovirus/Enterovirus was the most frequently identified agent (42.4%), followed by RSV (15.3%), SARS-CoV-2 (11.9%), and Adenovirus (10.2%). The other viruses were detected at more modest frequencies (Figure 7).
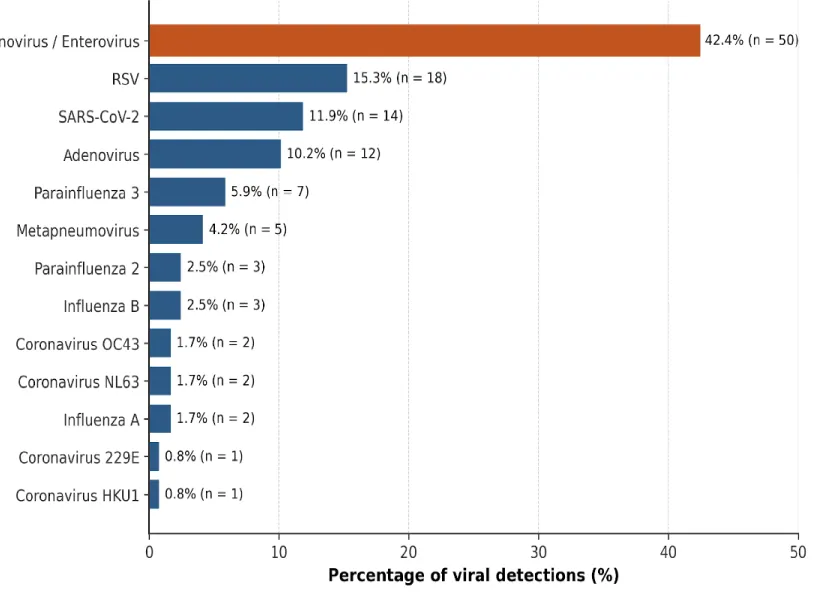
Figure 7: Frequency of viruses identified (n = 118 detections).
Bacterial presence was low (≈ 3% of samples): only four samples were positive for a bacterium.
Among these agents, Bordetella pertussis was the most frequently detected (n = 2). Mycoplasma pneumoniae and Chlamydia pneumoniae were each detected in one sample (Table 2).
| Table 2: Distribution of identified bacteria (n = 4 detections). | |
| Bacterium | Detections (n) |
| Bordetella pertussis | 2 |
| Mycoplasma pneumoniae | 1 |
| Chlamydia pneumoniae | 1 |
| Total | 4 |
Mono- and co-infections
Analysis of the 90 positive samples showed a predominance of mono-infections (64.4%). Viral co-infections accounted for nearly one-third of cases (31.1%), reflecting the concurrent circulation of several viral agents. Virus–bacterium co-infections remained rare (4.4%), confirming the predominance of viral etiologies (Figure 8).
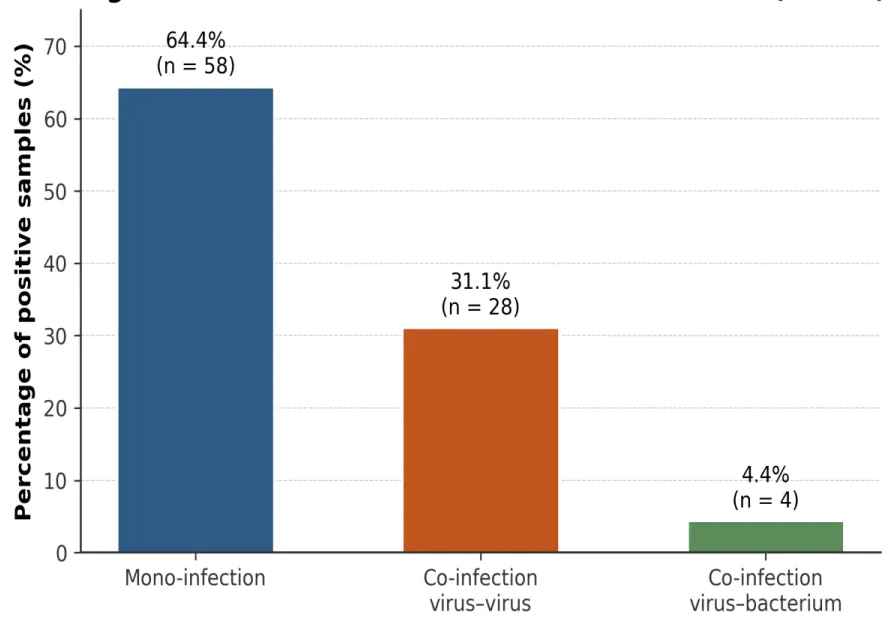
Figure 8: Distribution of mono- and co-infections (n = 90).
The distribution of mono- and co-infections by pathogen is detailed in Table 3 and illustrated in Figure 9.
| Table 3: Mono- and co-infections by pathogens. | ||||
| Pathogen | Type | Mono-infection (n) | Co-infection (n) | Total (n) |
| Rhinovirus / Enterovirus | Virus | 27 | 23 | 50 |
| RSV | Virus | 9 | 9 | 18 |
| SARS-CoV-2 | Virus | 7 | 7 | 14 |
| Adenovirus | Virus | 3 | 9 | 12 |
| Parainfluenza 3 | Virus | 3 | 4 | 7 |
| Metapneumovirus | Virus | 2 | 3 | 5 |
| Parainfluenza 2 | Virus | 1 | 2 | 3 |
| Influenza B | Virus | 2 | 1 | 3 |
| Coronavirus OC43 | Virus | 1 | 1 | 2 |
| Coronavirus NL63 | Virus | 1 | 1 | 2 |
| Influenza A | Virus | 2 | 0 | 2 |
| Coronavirus 229E | Virus | 0 | 1 | 1 |
| Coronavirus HKU1 | Virus | 0 | 1 | 1 |
| Bordetella pertussis | Bacterium | 0 | 2 | 2 |
| Chlamydia pneumoniae | Bacterium | 0 | 1 | 1 |
| Mycoplasma pneumoniae | Bacterium | 0 | 1 | 1 |
| Total | — | 58 | 66 | 124 |
| Note: the “Co-infection (n)” column totals 66 detections from 32 co-infected samples; each co-infected sample contains ≥ 2 agents, which is why the total number of detections exceeds the number of samples. | ||||
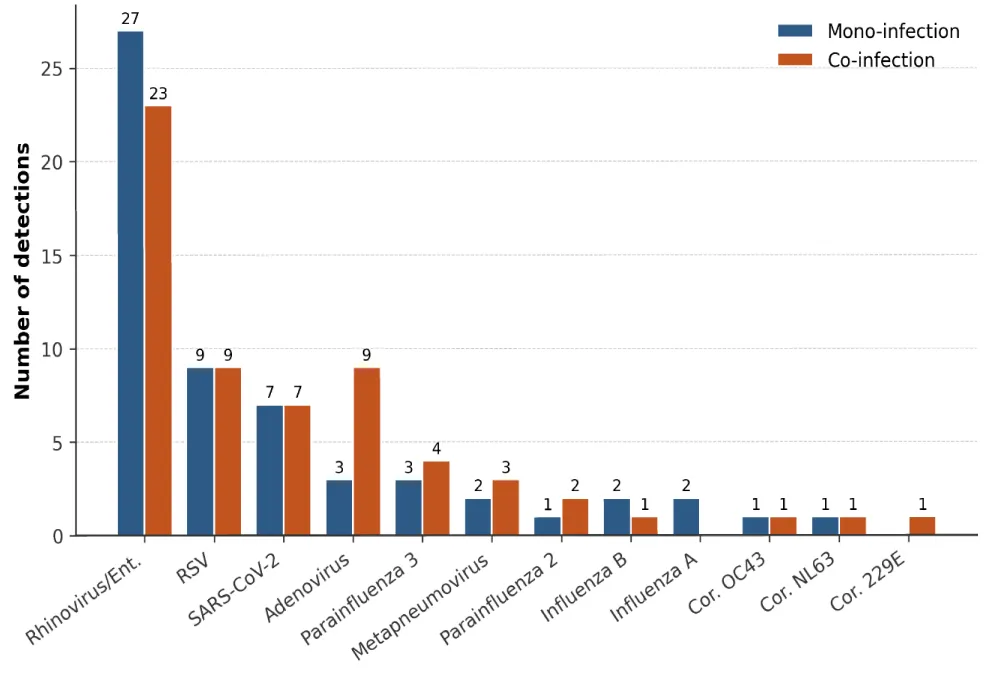
Figure 9: Mono vs. co-infections by viral agent.
Note: the “Co-infection (n)” column totals 66 detections from 32 co-infected samples; each co-infected sample contains ≥ 2 agents, which is why the total number of detections exceeds the number of samples.
Demographic characteristics
In our study, the age distribution shows a clear predominance of children aged 3 to 4 years (64.0%), followed by those aged 1 to 2 years (23.2%), whereas infants under one year and children aged 5 years were less represented (4.8% and 8.0%, respectively). This profile, centered on the preschool age, contrasts with the classical descriptions of pediatric respiratory infections, which are often dominated by infants.
Internationally, viral respiratory infections mainly affect children under five, with an incidence peak generally observed between 2 and 5 years, linked to increased exposure to community settings [5]. In Europe — notably in the Netherlands and Spain — multiplex PCR-based studies confirm strong viral activity in children aged 1 to 5 years, but with a more homogeneous distribution across age subgroups than in our series, which was marked by a concentration of cases between 3 and 4 years [6,7]. In the United States, respiratory illnesses requiring hospitalization mainly involve children under five, with a median age close to two years, reflecting a higher proportion of infants than in our cohort [8].
In Morocco, national data indicate a high frequency of acute lower respiratory infections in children under five, particularly between 6 and 23 months, which differs from our series, where this age group represented only about one quarter of patients, suggesting a divergence between population-based surveys and hospital-based observations [9]. These discrepancies could be explained by several factors, including variable hospitalization criteria, preferential referral of infants with severe forms to specialized centers, and more frequent use of respiratory multiplex PCR in preschool-aged children with recurrent or prolonged infections [10].
Sex
A male predominance was observed, with 72 boys (57.6%) versus 53 girls (42.4%), giving an M/F sex-ratio of 1.36. This finding is consistent with several international reports showing a male overrepresentation in pediatric viral respiratory infections: Malaysia (sex-ratio 1.4) [11], Italy (≈ 1.3) [12], China (1.2 to 1.5) [13,14], France (1.2) [15], and Morocco (male proportion 56–59%) [16]. However, this trend is not universal: a study from Cambodia reported a female predominance, with an M/F sex-ratio of 0.8 [17]. This male predominance could be explained by later immune maturation in boys, anatomical differences in the airways, and early hormonal influences.
Yearly trend
The strong concentration of samples in 2022/2023 (61.6%) likely reflects the post-COVID-19 epidemic peak, marked by intense viral circulation after the lifting of mitigation measures. This temporal dynamic, though variable across contexts, is consistent with international literature reporting that diagnostic activity related to respiratory multiplex PCR is closely dependent on seasonal viral circulation, epidemic cycles, and local management practices [11,18].
Multiplex PCR positivity rate
The 72% positivity rate observed is close to the high rates reported in hospital and epidemic contexts: Belgium (83.9%) [18], Italy (84.7%) [12], Cairo (93.8%) [19], and China (80.8%) [13], suggesting intense viral circulation and targeted clinical selection. Conversely, lower rates have been described in Turkey (48.2%) and the United States (45.9%), probably in connection with broader inclusion criteria or sampling outside seasonal peaks [20,21] (Figure 10).
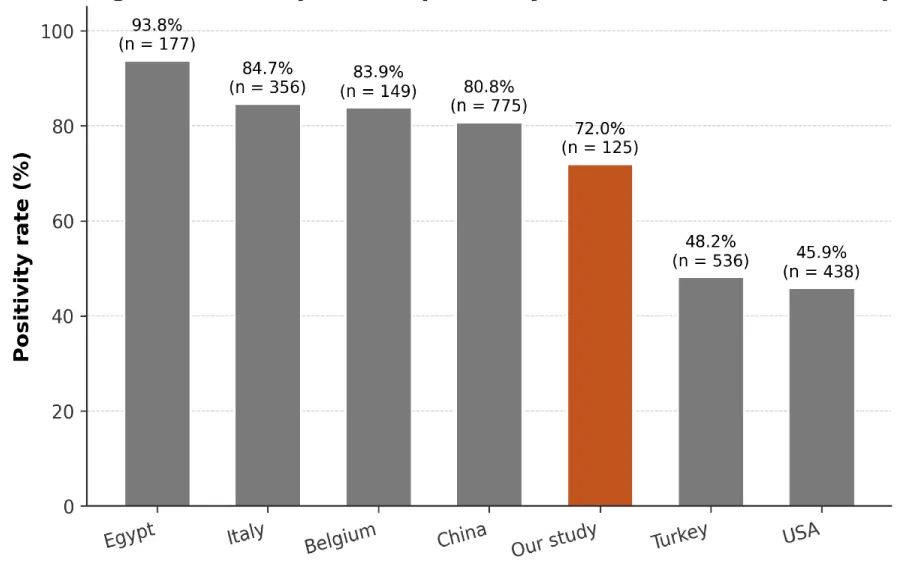
Figure 10: International comparison of multiplex PCR positivity rate.
Thus, the 72% positivity rate observed in our series occupies an intermediate position between the high values reported in contexts of intense viral circulation and the lower rates described in populations with more heterogeneous recruitment. It reflects both an appropriate use of multiplex respiratory PCR in our clinical practice and the epidemiological and organizational specificities of our study context.
Distribution of pathogens
In our cohort, 122 pathogens were identified among 90 positive samples, suggesting a notable frequency of co-infections. Viruses accounted for the majority of detections (96.7%; n = 118), versus only 3.3% bacterial detections (n = 4). This viral predominance is consistent with Moroccan data reporting 340 viral detections out of 387 positive samples in children hospitalized for severe acute respiratory infection [16]. It is also consistent with US data on pediatric community-acquired pneumonia, where bacteria are identified in only about 15% of children [21].
The viral distribution was dominated by Rhinovirus/Enterovirus (42.4%), followed by RSV (15.3%), SARS-CoV-2 (11.9%), and Adenovirus (10.2%), reflecting a characteristic pediatric profile. This Picornaviridae predominance is consistent with African data from Ghana and the Central African Republic, where their frequency reached approximately 36% and 40%, respectively [22,23]. Conversely, in France, RSV remains historically the main virus of winter respiratory infections, ahead of Rhinovirus, whereas Chinese data show a substantial joint circulation of Rhinovirus/Enterovirus and RSV [7,13]. The other viruses show frequencies broadly comparable to international data: Adenovirus at 10.2%, close to French and Chinese rates; human Metapneumovirus at 4.2%, close to French data; and Parainfluenza viruses at 8.4%, within the ranges reported internationally. In contrast, Influenza A/B (4.2%) and seasonal coronaviruses (3.4%) appear less frequent than in pre-pandemic series, likely related to post-COVID epidemiological changes, while the frequency of SARS-CoV-2 (11.9%) reflects the recent study period [7,13,22,23] (Figure 11).
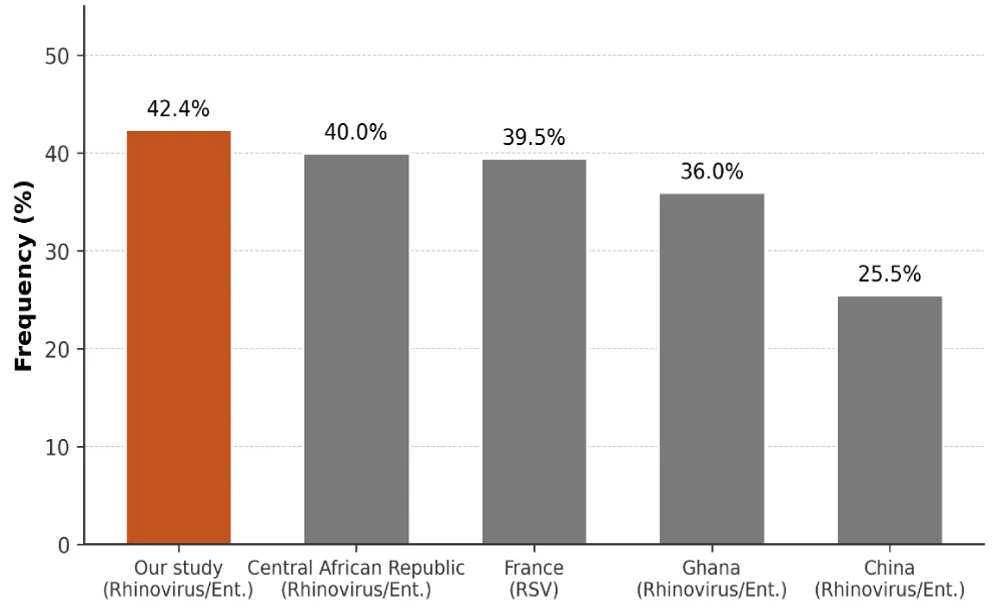
Figure 11: Most frequently identified respiratory virus — international comparison.
Detected bacteria
In our pediatric cohort, atypical bacteria were rarely detected, with only four cases: Bordetella pertussis (n = 2), Mycoplasma pneumoniae (n = 1), and Chlamydia pneumoniae (n = 1). This low frequency is consistent with the literature, which reports a generally limited contribution of atypical bacteria compared with viruses in pediatric respiratory infections. In China, a large pediatric series using the Film Array Respiratory Panel reported higher frequencies of Mycoplasma pneumoniae and Bordetella pertussis (10.6% and 6.3%) [13]. Conversely, a Swiss cohort of 4,460 children reported a Mycoplasma pneumoniae prevalence of only 1.6%, close to our results [24].
For Chlamydia pneumoniae, a Mexican study in children hospitalized for pneumonia reported a higher frequency of 16.2%, probably related to a targeted selection of documented pneumonias [25]. Thus, despite possible underestimation due to the limited size of our sample, our results confirm the viral predominance and the secondary role of atypical bacteria in pediatric respiratory infections, particularly outside confirmed community-acquired pneumonias.
Respiratory co-infections
Co-infections concerned 35.6% of positive samples, with a clear predominance of viral co-infections (31.1%) and a low proportion of virus–bacterium associations (4.4%). This frequency is consistent with international pediatric data: 30 to 40% in Belgium [26], 25 to 35% in France [7], 33% in China [13], and about one-third in the United States [27]. The low frequency of virus–bacterium co-infections observed in our series is also consistent with the literature, which describes these associations as less frequent in pediatric respiratory infections of predominantly viral etiology [28]. Thus, our results fit within international trends and could be explained by the young age of patients, the seasonality of respiratory viruses, and the high sensitivity of the molecular techniques used.
Study limitations
Our study has certain methodological limitations that must be acknowledged. First, its retrospective design makes it susceptible to inherent selection bias and missing data. Second, this is a single-center study, which may limit the external validity and generalizability of our findings to other populations. Therefore, large-scale, prospective, multicenter studies are required to validate our conclusions.
This work highlights the value of respiratory multiplex PCR in the etiological diagnosis of pediatric respiratory infections at Mohammed V Military Teaching Hospital in Rabat. The use of the Film Array Respiratory Panel made it possible to rapidly identify a broad spectrum of respiratory pathogens — mainly viral — and to improve the interpretation of biological markers such as CRP and leukocyte count, which are often non-specific in children. The dominant role of Rhinovirus/Enterovirus (42.4%) in our post-COVID Moroccan cohort confirms the emerging international trend and represents the most original finding of our series.
This syndromic approach contributes to earlier and better-targeted management by guiding isolation measures, facilitating the initiation of appropriate treatment, and limiting inappropriate antibiotic use. However, its optimal integration into clinical practice requires precise recommendations to rationalize its indications, given its high cost. Finally, sustained virological surveillance appears essential to better understand the dynamics of respiratory pathogens, adapt diagnostic strategies, and anticipate epidemic episodes.
Declarations
Funding: This work received no specific funding.
Conflicts of interest: The authors declare that they have no conflicts of interest related to this article.
Author contributions
Anouar Akhssas: Conceptualization, investigation, visualization, writing — original draft, editing, and validation.
Elarbi Bouaiti: Project administration and validation.
Mohamed-Rida Tagajdid: Project administration and validation.
Hicham Elannaz: Project administration and validation.
Salma Hassine: Project administration and validation.
Soukaina Ouannass: Project administration and validation.
Ahmad Reggad: Project administration and validation.
Mohamed Elqatni: Project administration and validation.
Z. Kasmi: Project administration and validation.
Abdelilah Laraqui: Project administration and validation.
N. Touil: Project administration and validation.
B. Machichi: Project administration and validation.
Abdelilah Radi: Project administration and validation.
Hakim Ourrai: Project administration and validation.
Rachid Abilkassem: Supervision, project administration, and validation.
Mostapha Elouennass: Supervision, project administration, and validation.
Khalid Ennibi: Supervision, project administration, and validation.
I. Lahlou Amine: Supervision, project administration, and validation.
Rachid Abi: Writing — review & editing, supervision, and validation.
- Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C. Estimates of world-wide distribution of child deaths from acute respiratory infections. The Lancet Infectious Diseases. 2002;2(1):25-32. Available from: https://doi.org/10.1016/s1473-3099(01)00170-0
- Ministry of Health, Kingdom of Morocco. Santé en chiffres 2022 [Internet]. Rabat: Ministry of Health; 2024 [cited 2026 May 25]. Available from: https://www.sante.gov.ma/Documents/2024/02/Sante%20en%20chiffre%202022%20VF1.pdf
- Chen YS, Liu PY, Huang YF, Chen CS, Chiu LH, Huang NY, et al. Comparison of diagnostic tools with multiplex polymerase chain reaction for pediatric lower respiratory tract infection: a single-center study. Journal of Microbiology, Immunology and Infection. 2013;46(6):413-418. Available from: https://doi.org/10.1016/j.jmii.2012.07.016
- bioMérieux. BIOFIRE® FILMARRAY® [Internet]. Available from: https://www.biomerieux.com
- Monto AS. Viral respiratory infections in the community: epidemiology, agents, and interventions. The American Journal of Medicine. 1995;99(6B):24S-27S. Available from: https://doi.org/10.1016/s0002-9343(99)80307-6
- Wishaupt JO, Van Der Ploeg T, De Groot R, Versteegh FGA, Hartwig NG. Single- and multiple viral respiratory infections in children: disease and management cannot be related to a specific pathogen. BMC Infectious Diseases. 2017;17(1):62. Available from: https://doi.org/10.1186/s12879-016-2118-6
- Mengelle C, Mansuy JM, Pierre A, Claudet I, Grouteau E, Micheau P, et al. The use of a multiplex real-time PCR assay for diagnosing acute respiratory viral infections in children attending an emergency unit. Journal of Clinical Virology. 2014;61(3):411-417. Available from: https://doi.org/10.1016/j.jcv.2014.08.023
- Jain S, Williams DJ, Arnold SR, Ampofo K, Bramley AM, Reed C, et al. Community-acquired pneumonia requiring hospitalization among U.S. children. The New England Journal of Medicine. 2015;372(9):835-845. Available from: https://doi.org/10.1056/nejmoa1405870
- Bennani Mechita N, Razine R, Elmarnissi A, Lahlou L, Cherkaoui I, Lyaghfouri A, et al. Évolution des infections respiratoires aiguës basses chez les enfants âgés de moins de 5 ans au Maroc. Revue d'Épidémiologie et de Santé Publique. 2017;65(Suppl 2):S72-S73. Available from: https://doi.org/10.26719/emhj.20.122
- Jroundi I, Mahraoui C, Benmessaoud R, Moraleda C, Benjelloun B, Bassat Q. Knowledge gaps on paediatric respiratory infections in Morocco, Northern Africa. Archives of Public Health. 2015;73(1):28. Available from: https://doi.org/10.1186/s13690-015-0076-x
- Khor CS, Sam IC, Hooi PS, Quek KF, Chan YF. Epidemiology and seasonality of respiratory viral infections in hospitalized children in Kuala Lumpur, Malaysia: a retrospective study of 27 years. BMC Pediatrics. 2012;12:32. Available from: https://doi.org/10.1186/1471-2431-12-32
- Ciotti M, Maurici M, Santoro V, Coppola L, Sarmati L, De Carolis G, et al. Viruses of respiratory tract: an observational retrospective study on hospitalized patients in Rome, Italy. Microorganisms. 2020;8(4):501. Available from: https://doi.org/10.3390/microorganisms8040501
- Li J, Tao Y, Tang M, Du B, Xia Y, Mo X, et al. Rapid detection of respiratory organisms with the Film Array respiratory panel in a large children's hospital in China. BMC Infectious Diseases. 2018;18(1):510. Available from: https://doi.org/10.1186/s12879-018-3429-6
- Deng J, Ma Z, Huang W, Li C, Wang H, Zheng Y, et al. Respiratory virus multiplex RT-PCR assay sensitivities and influence factors in hospitalized children with lower respiratory tract infections. Virologica Sinica. 2013;28(2):97-102. Available from: https://doi.org/10.1007/s12250-013-3312-y
- Koenig-Zores C, Stoll-Keller F, Ammouche C, Donato L. L'analyse virologique des aspirations nasopharyngées reflète-t-elle l'infection respiratoire basse chez l'enfant? Étude en PCR multiplex. Revue Française d'Allergologie. 2013;53(2):59-64. Available from: https://doi.org/10.1016/j.reval.2012.11.007
- Lamrani Hanchi A, Guennouni M, Rachidi M, Benhoumich T, Bennani H, Bourrous M, et al. Epidemiology of respiratory pathogens in children with severe acute respiratory infection and impact of the multiplex PCR Film Array respiratory panel: a 2-year study. International Journal of Microbiology. 2021;2021:2276261. Available from: https://doi.org/10.1155/2021/2276261
- Ly N, Tokarz R, Mishra N, Sameroff S, Jain K, Rachmat A, et al. Multiplex PCR analysis of clusters of unexplained viral respiratory tract infection in Cambodia. Virology Journal. 2014;11(1):224. Available from: https://doi.org/10.1186/s12985-014-0224-x
- Busson L, Bartiaux M, Brahim S, Konopnicki D, Dauby N, Gérard M, et al. Contribution of the Film Array respiratory panel in the management of adult and pediatric patients attending the emergency room during 2015-2016 influenza epidemics: an interventional study. International Journal of Infectious Diseases. 2019;83:32-39. Available from: https://doi.org/10.1016/j.ijid.2019.03.027
- Gad NM, Refaay D, Gad NM, Mohamed ZAZ. Viral infections in Egyptian hospitalized children with acute respiratory tract infections. Journal of Clinical & Cellular Immunology. 2017;8(5). Available from: https://www.longdom.org/open-access/viral-infections-in-egyptian-hospitalized-children-with-acute-respiratory-tract-infections-51913.html
- Keske Ş, Ergönül Ö, Tutucu F, Karaaslan D, Palaoğlu E, Can F. The rapid diagnosis of viral respiratory tract infections and its impact on antimicrobial stewardship programs. European Journal of Clinical Microbiology & Infectious Diseases. 2018;37(4):779-783. Available from: https://doi.org/10.1007/s10096-017-3174-6
- Katz SE, Williams DJ. Pediatric community-acquired pneumonia in the United States. Infectious Disease Clinics of North America. 2018;32(1):47-63. Available from: https://doi.org/10.1016/j.idc.2017.11.002
- Wilson PT, Baiden F, Brooks JC, Giessler KM, Apio G, Punguyire D, et al. Respiratory pathogens in children 1 month to 5 years of age presenting with undifferentiated acute respiratory distress in 2 district-level hospitals in Ghana. Journal of the Pediatric Infectious Diseases Society. 2019;8(4):361-364. Available from: https://doi.org/10.1093/jpids/piy090
- Bobossi Serengbe G, Gody JC, Fioboy R, Nakoune E. Viral etiology of acute respiratory infections in children in Bangui. Archives de Pédiatrie. 2015;22(3):324-325.
- Dierig A, Hirsch HH, Decker M, Bielicki JA, Heininger U, Ritz N. Mycoplasma pneumoniae detection in children with respiratory tract infections and influence on management—a retrospective cohort study in Switzerland. Acta Paediatrica. 2020;109(2):375-380. Available from: https://doi.org/10.1111/apa.14891
- Merida Vieyra J, De Colsa Ranero A, Palacios Reyes D, Murata C, Aquino Andrade A. Chlamydophila pneumoniae-associated community-acquired pneumonia in paediatric patients of a tertiary care hospital in Mexico: molecular diagnostic and clinical insights. Scientific Reports. 2023;13(1):21477. Available from:
- Litwin CM, Bosley JG. Seasonality and prevalence of respiratory pathogens detected by multiplex PCR at a tertiary care medical center. Archives of Virology. 2014;159(1):65-72. Available from: https://doi.org/10.1007/s00705-013-1794-4
- Martin ET, Kuypers J, Wald A, Englund JA. Multiple versus single virus respiratory infections: viral load and clinical disease severity in hospitalized children. Influenza and Other Respiratory Viruses. 2012;6(1):71-77. Available from: https://doi.org/10.1111/j.1750-2659.2011.00265.x
- Mahony JB. Detection of respiratory viruses by molecular methods. Clinical Microbiology Reviews. 2008;21(4):716-747. Available from: https://doi.org/10.1128/cmr.00037-07